
PO64 | A silent hemorrhage in the immuno-thrombotic chaos of antiphospholipid syndrome
G. Autiero, S.A. Malerba, A. Malaguti, M. Dalla Vestra, F. Presotto | Medicina Generale, Ospedale dell’Angelo, Mestre-Venezia, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background: Adrenal insufficiency is a rare but potentially life-threatening complication of the antiphospholipid antibody syndrome (APS). Adrenal failure typically follows prior thromboembolic manifestations of APS. Although bleeding is uncommon, both thrombotic and hemorrhagic events can occur concurrently in catastrophic APS (CPAS). Hemorrhagic diathesis may result from micro-thrombotic events, sever thrombocytopenia or hypothrombinemia.
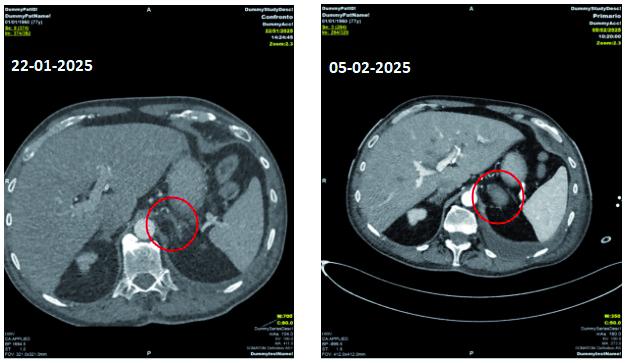
Case report: A 77-year-old male with a medical history of arterial hypertension and diabetes mellitus was admitted to the Cardiology Unit of the Ospedale dell’Angelo in Mestre-Venice in January 2025 for an intermediate-high risk saddle pulmonary embolism associated with deep vein thrombosis of lower limbs. In the two weeks before the admission he experienced dry cough, fever and rhinitis. Anticoagulant therapy with unfractionated heparin was started, however, aPTT values remained below the therapeutic range. Empirical antibiotic therapy was also administered due to the elevated inflammatory markers (C-reactive protein 234 mg/L and procalcitonin 0,7 mcg/L) and the presence of pulmonary consolidation on the chest Computed Tomography scan. During hospitalization, the patient’s clinical conditions progressively deteriorated, presenting hypotension, anemia, acral ischemia and worsening of respiratory failure. Radiological imaging revealed bilateral adrenal enlargement consistent with hemorrhage, which was larger at the left side. Furthermore, due to secondary acute kidney failure with oligo-anuria, the patient was transferred to the intensive care unit where continuous veno-venous ultrafiltration (CVVH) was initiated. In consideration of bleeding and anemia, anticoagulant therapy was temporary reduced and an inferior vena cava (IVC) filter was placed. Blood tests showed triple positivity for lupus anticoagulant (LAC), anti-B2 glycoprotein and anti-cardiolipin (at high titers) strongly suggestive of CAPS. Subsequently, the thrombotic diathesis was treated with antiplatelet therapy, prostanoids and anticoagulant therapy with Warfarin. At the same time, immunosuppressive treatment with high dose corticosteroids and a 5-day cycle of plasmapheresis were administered, with progressive clinical improvement. At a predetermined time after discontinuation of corticosteroid therapy, serum cortisol levels and ACTH tests were performed and confirmed impaired adrenal function. Replacement therapy with cortisone acetate was started. A whole body PET-CT scan was performed which showed no images suspicious for cancer. At the immunological follow-up approximately 3 months later, the diagnosis of antiphospholipid antibody syndrome was confirmed with high-titer positivity of antiphospholipid antibodies and the patient will be followed up at the Thrombotic and Hemorrhagic disease clinic.
Conclusions: CAPS is a rare variant of APS characterized by micro- and/or macrothrombi in multiple organs. It is commonly triggered by several factors including infections, trauma, surgery, cancer or the discontinuation of oral anticoagulation. The occurrence of mono-bilateral adrenal hemorrhage, as described in this report, is exceptional. This case highlights that adrenal hemorrhage can be part of the thrombotic complications associated with both primary and secondary APS that, if misdiagnosed, may lead to a life-threatening acute adrenal failure.
Figure 1.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


