
PO79 | Trying to hit the hit in the shadow of renal failure: a complex case managed with danaparoid
S. Chessa1,2, M. Anedda2, M.V. Cherchi2, M. Vacca1,2, M. Caboni2, J. Pilia2, A.M. Bussu2, M. Mantega2, G. Costanzo1, D. Firinu1, S. Del Giacco1, A. Mameli3, D. Barcellona3 | 1Department of Medical Science and Public Health, University of Cagliari; 2Internal Medicine, ASL Sulcis, PO Sirai, Carbonia; 3Department of Medical Sciences and Public Health, Hemostasis and Thrombosis Unit, University of Cagliari and AOU of Cagliari, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background: Heparin-induced thrombocytopenia (HIT) type II is a rare, immune-mediated adverse effect of heparin exposure, caused by antibodies against PF4-heparin complexes. These trigger platelet activation and can lead to life-threatening thrombosis. Managing HIT is challenging: anticoagulation is mandatory despite thrombocytopenia. In hemodialysis patients, who are frequently exposed to heparin and have limited alternatives due to renal clearance, clinical decisions are often complex. Early recognition is key to avoiding complications.
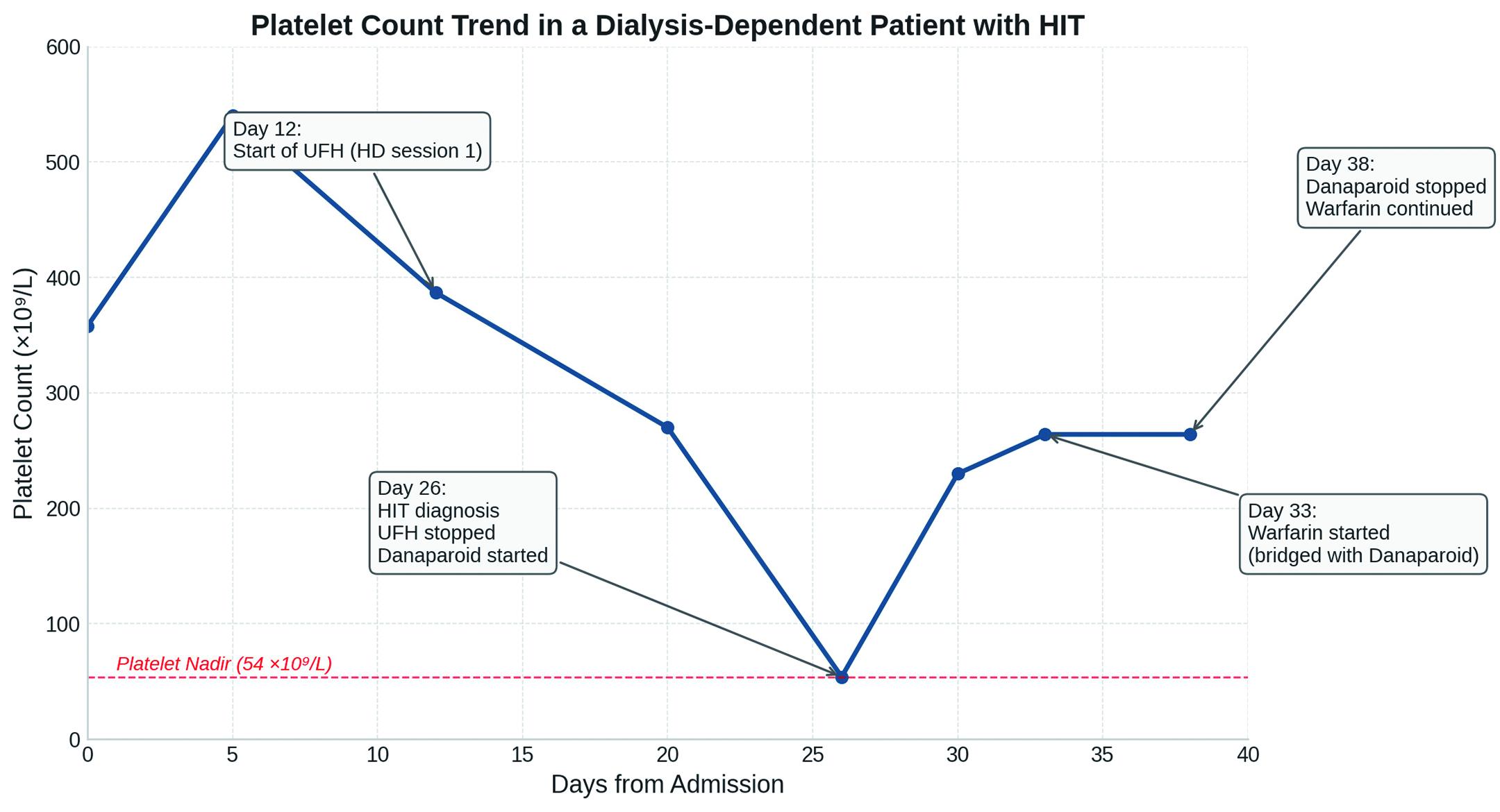
Case Report: An 88-year-old woman was admitted for E. coli urosepsis. Her past medical history included chronic kidney disease, without any prior heparin exposure. Initial platelet count was 358×109/L. On day 12, worsening oligoanuric renal failure (eGFR 6 mL/min) required hemodialysis with unfractionated heparin. Seven days later, the platelet count started to drop (day 20: 274×109/L) rapidly reaching a nadir of 54×109/L on day 26. As infection had resolved and antibiotics were stopped, HIT was suspected (4T score: high probability). Despite the absence of overt symptoms, a Doppler ultrasound showed right femoral vein thrombosis, near the dialysis catheter. Anti-PF4 antibodies were positive (EIA: 7.4 U/mL; cutoff >1 U/mL). UFH was stopped immediately. Given ongoing dialysis needs and limited drug availability, we consulted a thrombosis expert and the HIT-THE-HIT network. The choice of drug was complicated by the fact that in our peripheral hospital access to certain medication is limited, as is the ability to monitor their activity in the laboratory. The choice fell on danaparoid. In patients on hemodialysis, danaparoid dosing depends on weight and session frequency. In our case, 3750 units were administered before each session, with prior monitoring of anti-Xa activity, which showed no evidence of drug buildup. Platelet count normalized in five days. Clinical stability improved and total body CT scan showed no signs of venous or arterial thrombosis elsewhere. As platelet levels rose – likely reflecting decreased anti-PF4 activity - warfarin was initiated on day 5. Danaparoid was stopped at day 11, when INR was therapeutic. Figure 1 illustrates the progression of platelet counts throughout the patient’s hospital stay. Unfortunately, the patient later died of septic shock unrelated to HIT. Nonetheless, thrombocytopenia and thrombosis were successfully managed without further complication.
Conclusions: This case illustrates a critical diagnostic and therapeutic challenge: the need to anticoagulate a thrombocytopenic, dialysis-dependent patient in a setting with limited pharmacologic options. The simultaneous presence of thrombosis and falling platelets requires swift, structured assessment and confident clinical decision-making. Danaparoid allowed us to bridge dialysis safely while achieving hematologic recovery. Clinical suspicion, even in the absence of overt symptoms, was key. Unexplained platelet drops in dialysis patients should always prompt evaluation for HIT. Prompt recognition and tailored anticoagulation can change the course of this potentially fatal complication.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


