
PO80 | Heparin-induced thrombocytopenia: a monocentric experience with danaparoid
L. D’Innocenzo, S. Sorrentino, M. De Siati, A. Ferretti, E. De Candia | Unit of Haemostasis and Thrombosis Diseases, Fondazione Policlinico Universitario A. Gemelli, IRCCS, Roma, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background: Heparin-induced thrombocytopenia (HIT) is a severe immune-mediated complication of heparin therapy, with significant thrombotic risk. Anti-PF4 antibodies may develop in up to 8% of exposed patients, but only 1–5% progress to clinical HIT. Early withdrawal of heparin and prompt initiation of a non-heparin anticoagulant are essential to manage this complication. Sodium danaparoid, a heparinoid with high anti-Xa activity and low anti-PF4 cross-reactivity, can inhibit PF4–heparin–IgG complex formation, limiting platelet (PLT) activation. It is the only anticoagulant approved for venous thrombosis prophylaxis in patients with previous HIT.
Aims andMethods: We report five HIT cases diagnosed with 4T score ≥4, positive immunologic anti-PF4 IgG (HemosIL Acustar), and positive functional test (P-selectin expression by flow cytometry). Heparin was discontinued and danaparoid was initiated, followed by oral anticoagulation. Bridging with argatroban was used in unstable patients or those with high surgical risk.
Case #1: 74-y.o. woman post mitral valve replacement, exposed to unfractionated heparin (UFH) and low molecular weight heparin (LMWH), developed thrombocytopenia (nadir 48 x109/L), confirmed HIT. Treated with intravenous (IV) and subcutaneous (SC) danaparoid with PLT recovery >150x109/L in 5 days and safe transition to warfarin.
Case #2: 64-y.o. man after mitral valve surgery, exposed to UFH/LMWH, developed HIT (nadir 59x109/L). Initially treated with IV argatroban, then switched to SC danaparoid. PLT count normalized in 5 days, with safe warfarin initiation.
Case #3: 93-y.o. woman post-hip arthroplasty, exposed to LMWH for new-onset atrial fibrillation, developed HIT (nadir 34x109/L) with concurrent deep vein thrombosis and pulmonary embolism. She was treated with IV danaparoid (PLT to 121x109/L after 5 days), then discontinued erroneously with subsequent count drop (28 x109/L), but recovered >150 x109/L in 6 days after SC danaparoid reintroduction, then safely switched to apixaban.
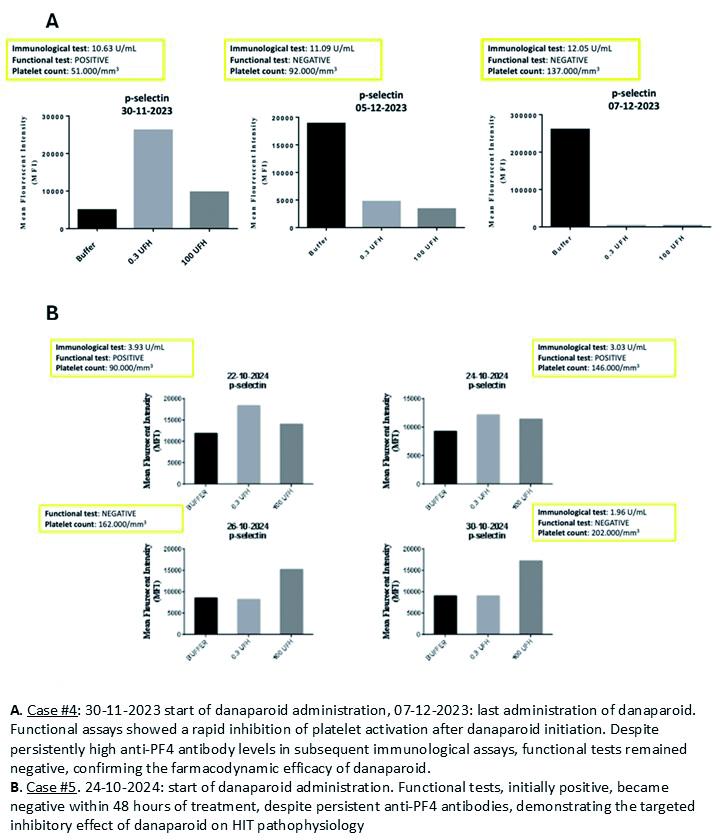
Case #4: 74-y.o. woman post-mitral valve replacement and tricuspid repair, exposed to UFH developed severe thrombocytopenia (nadir 18x109/L), high-titer anti-PF4 antibodies (25.25 U/mL), and jugular thrombosis. Fondaparinux was started but stopped due to a further PLT drop. IV corticosteroids led to a slight rise in PLT count, allowing initiation of IV argatroban. Once clinically stable, the patientstarted SC danaparoid, with gradual PLT count recovery (at discharge was >130 x109/L) and safe transition to warfarin.
Case #5: 60-y.o. man post-emergency valve surgery for myocardial infarction with papillary muscle rupture who developed HIT, exposed to UFH and LMWH, with prosthetic valve thrombosis (anti-PF4 3.93 U/mL, nadir 126 x109/L). Treated with danaparoid, PLT count rose to 202x109/L over 8 days and warfarin was then initiated safely.
Results: Four patients reached PLT count >150 x109/L within 5–10 days; case #4 in 20 days. No thrombotic or bleeding complications occurred. In cases #4 and #5, repeated functional testing showed rapid loss of PLT activation after danaparoid, despite persistent immunological anti-PF4 IgG testing. This mismatch confirmed danaparoid effect on immune complex disruption.
Conclusions: Danaparoid is an effective and safe drug for HIT. Despite EMA approval and guidelines support, its use in Italy remains limited. Its low cross-reactivity and ability to interfere with immune complex formation support its use as a first-line therapy.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


