
PO34 | A negative oncologic follow up doesn’t always really mean no cancer: two case report of cancer-associated thrombotic microangiopathy
E. Cosi, A. Bertomoro, G. Bogoni, I. Bertozzi, I. Cortella, P. Simioni | Clinica Medica ORI, Azienda Ospedale-Università Padova, DIDAS, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background: Cancer-associated thrombotic microangiopathy (CA-TMA) is a rare but severe complication of malignancy characterized by microangiopathic hemolytic anemia (MAHA), thrombocytopenia, and organ dysfunction, typically in the absence of thrombotic thrombocytopenic purpura (TTP)-defining ADAMTS13 deficiency. Its pathophysiology is poorly understood, but it is hypothesized to involve direct endothelial injury by tumor cells, cytokine-mediated microvascular damage, or tumor-related procoagulant activity. Most cases of CA-TMA have been reported in patients with mucin-producing adenocarcinoma (e.g. gastric, breast cancer) and in those with disseminated malignancies, but also described in cases with isolated invasion of the bone marrow. Treatment primarily focuses on controlling the underlying malignancy; plasma exchange (PEX) and steroids, commonly used in TTP, are generally ineffective in CA-TMA. Prognosis remains poor, often due to advanced-stage malignancy and limited responsiveness to oncologic treatment. Prompt recognition and accurate diagnosis, including consideration of bone marrow biopsy (BMB), are critical for optimal management.
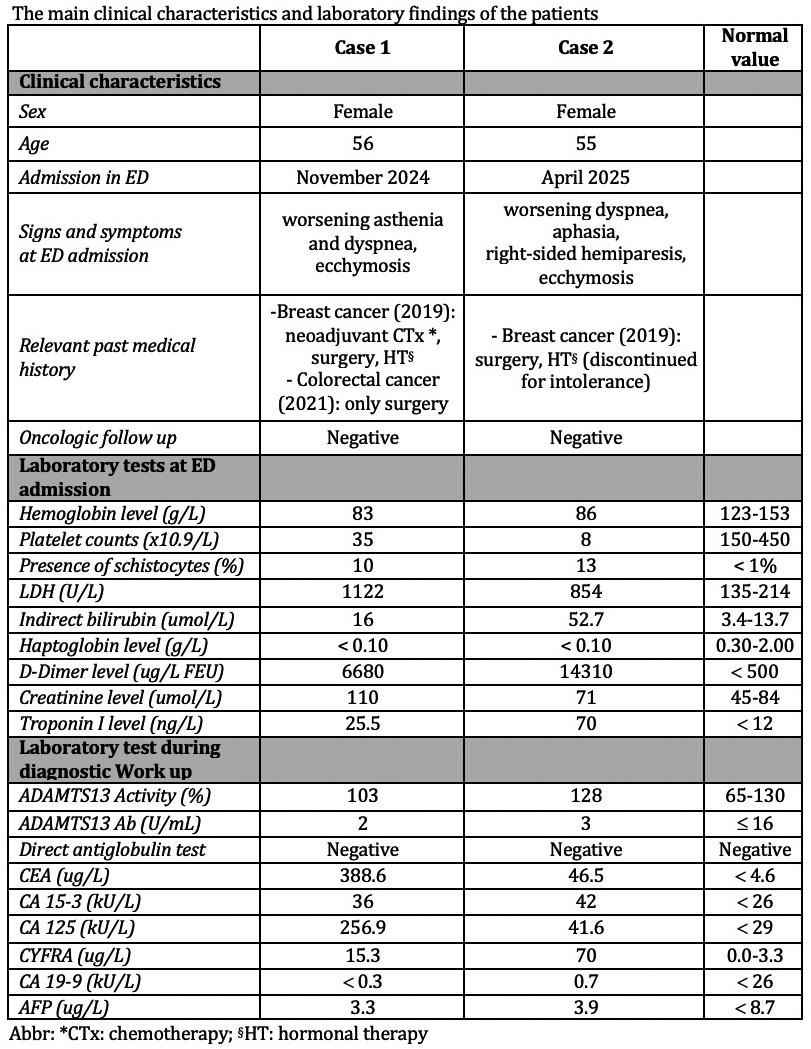
Case Report: We present two very similar cases of CA-TMA referred to our Department. The main clinical characteristics and laboratory findings of the patients are summarized in Table 1. In both cases, laboratory tests performed in the Emergency Department (ED) revealed severe thrombocytopenia and MAHA, so they were admitted to our Centre under the suspicion of TTP, and PEX and corticosteroids were initiated while awaiting ADAMTS13 activity results; in light of the normal levels of ADAMTS13 activity, TTP was ruled out and PEX discontinued; further investigation was pursued to identify alternative causes of TMA. In Case 1 a total-body CT scan and a colonoscopy were performed and found to be essentially unremarkable. In Case 2, a total-body CT scan, initially performed to rule out pulmonary embolism, revealed sternal osteolytic lesions and recent left rib fractures (she reported a recent car accident). Consequently, a PET-CT scan was obtained, showing widespread skeletal hypermetabolism. Given the non-definitive clinical presentation, both patients underwent BMB which revealed diffuse osteomedullary metastases of epithelial malignant neoplasm consistent with breast cancer, confirming the diagnosis of CA-TMA. Both patients were transferred to the Oncology Department to initiate chemotherapy, but despite rapid intervention, both patients died within 40 days (Case 1) and 6 days (Case 2) from admission.
Conclusions: CA-TMA is a life-threatening but often underrecognized manifestation of malignancy. CA-TMA does not respond to PEX or immunosuppressive therapy, for this reason early identification and differentiation from other TMAs, especially TTP, are essential. Diagnosis requires clinical suspicion and comprehensive evaluation, including imaging and BMB, especially when other diagnostic findings are inconclusive. Our cases highlight the critical role of early BMB in establishing diagnosis and initiating appropriate oncologic treatment. Literature review confirms the limited efficacy of supportive therapy alone and underscores the urgent need for targeted cancer therapy in improving survival. A multidisciplinary approach and awareness of CA-TMA in patients with known or suspected malignancy presenting with MAHA and thrombocytopenia can significantly influence diagnostic timelines and therapeutic strategies.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


