
PO24 | Emicizumab prophylaxis and bleeding outcomes: a single center clinical experience
A. Taglietti1, S. Ligia1, F. Paoletti1, R. Mormile1, E. Baldacci2, A. Chistolini1, C. Santoro1,2 | 1Hematology, Department of Translational and Precision Medicine, Sapienza University of Roma; 2Hematology, Azienda Ospedaliera Universitaria Policlinico Umberto I, Roma, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background and Aims: Emicizumab for hemophilia A (HA) has been increasingly employed in clinical practice. The aim is describing our real-world experience and clinical outcomes in severe HA patients (pts).
Methods: Retrospective, single-center study including severe HA pts, with/without inhibitors, with 6-month minimum follow-up (FU) since emicizumab start. Clinical data were collected from clinical charts and all participants signed an informed consent form.
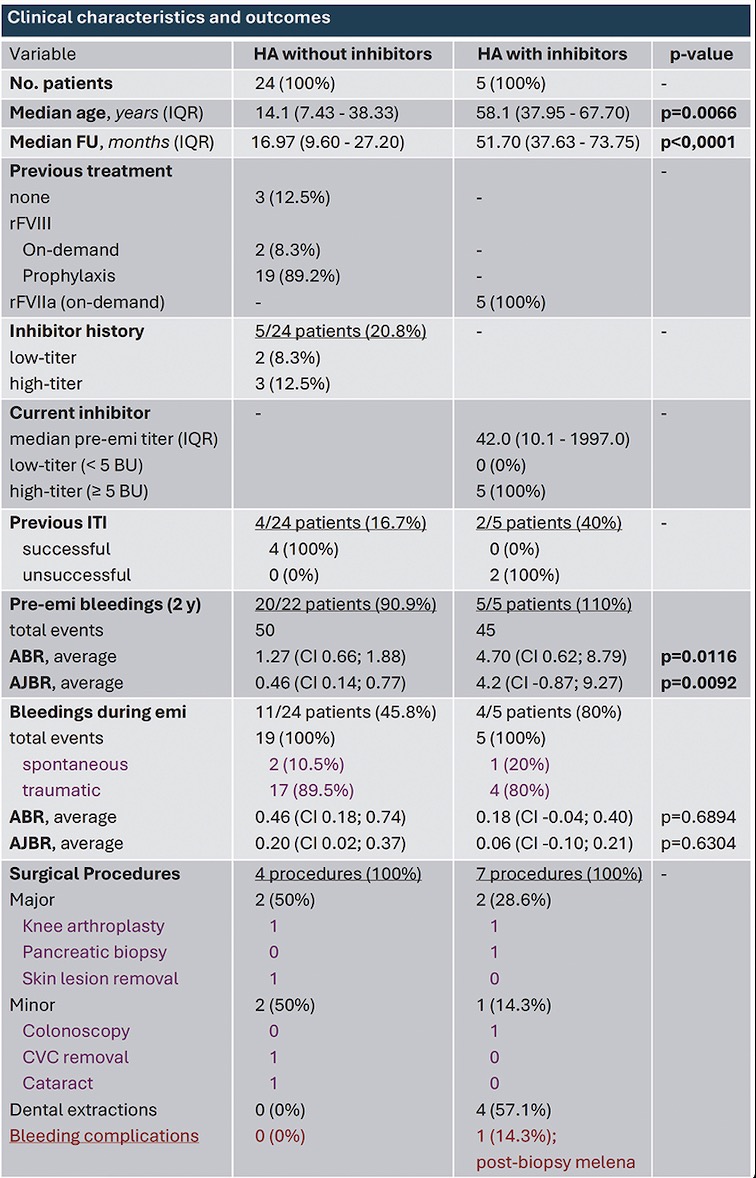
Results: We enrolled 29 severe HA pts who switched to emicizumab prophylaxis (EP). The only adverse event we recorded was a local skin reaction in 1 pt after his 1st emicizumab dose. Non-Inhibitor patients: 24 pts (82.8%), whose median age at switch was 14.1 years (7.43-38.33; min 0.65-max 55.33) and median FU is 16.97 months (9.6-27.2). Before EP, 3 (12.5%) were therapy naive, 2 (8.3%) treated on-demand, 19 (79.2%) were on recombinant factor VIII (rFVIII) prophylaxis. The main reasons for switching were achieving better bleeding control, avoiding intravenous infusion, and improving compliance. During EP, 1 pediatric pt, who had previously received few rFVIII infusions, developed an inhibitor following a traumatic injury that required rFVIII treatment. Patients with inhibitors (PwI): 5 pts (17.2%), whose median age at switch was 58.1 years (37.95-67.7) and median FU is 51.7 months (37.63- 73.75). All were treated with on-demand recombinant activated factor VII (rFVIIa). Procedures: during EP, 11 procedures were performed in 7 (13.8%) pts (4 PwI, 3 non-inhibitor): 4 major surgeries, 3 minor ones, 4 dental extractions. Major surgeries were managed with rFVIII/FVIIa, yet 1 PwI presented postoperative bleeding complications (melena after pancreatic biopsy) that required transfusions and large amounts of rFVIIa. Bleedings: During the 2 years prior to switch, 25 (85.2%) pts experienced at least one bleeding episode (5 PwI and 20 non-inhibitor). Comparing the mean annualized bleeding rate (ABR) and annualized joint bleeding rate (AJBR), PwI had significantly higher rates (p=0.0116 and p=0.0092). During EP, 14/29 (48.3%) pts never experienced a bleeding episode. 11 non-inhibitor pts experienced 19 mild-moderate bleeds: 17 traumatic and 2 spontaneous hematuria (same pt), all managed with rFVIII therapy. 4 PwI experienced a total of 5 mild-moderate bleeds: 4 traumatic (managed with rFVIIa) and 1 small spontaneous hematoma. Comparing pre-vs-post emicizumab ABR and AJBR, we observed a reduction by 63.78% (p=0.0114) and 56.52% (p=0.17) in the non-inhibitor group and a reduction by 96.17% (p=0.0079) and 98.57% (p=0.0476) in PwI. No significant difference was found in ABR and AJBR between PwI and non-inhibitor during EP (p=0.69 and p=0.63, respectively). During EP, ABR and AJBR did not differ between pediatric (age<12 years, 11 pts) and adult pts (age>12 years, 18 pts).
Conclusions: Despite our small cohort, we confirmed emicizumab efficacy and safety in severe HA pts with/without inhibitor. The different age and FU between the pt groups depend on timelines of regulatory indications for prescription. Only 2 pts had mild spontaneous bleeds and traumas were all easily managed. 1 PwI had severe bleeding after a high-risk procedure, despite additional rFVIIa. We found no significant differences in bleeding rates between pt groups during EP. We believe that the smaller AJBR reduction in the non-inhibitor group may be explained by a more confident approach to physical activity by pediatric pts.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


