
PO86 | Emicizumab in patients with moderate hemophilia A and severe bleeding phenotype: single-center real-world experience
A.L. Faccini, M. Biglietto, S. Sorella, E. Crisanti, M. Antonacci, R. Mormile, R. Ciciani, E. Baldacci, C. Santoro, S. Ligia | Hematology, Department of Translational and Precision Medicine Sapienza University of Roma, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background and Aims: The role of prophylaxis in moderate hemophilia A (HA) patients is less clear than in severe HA, given their variable bleeding phenotype. A relevant portion of moderate HA patients may have a severe bleeding phenotype, characterized by frequent hemarthrosis, with a consequent high risk of developing chronic arthropathy. Therefore, this patients’ subgroup has been historically managed with factor VIII (FVIII) prophylaxis. Recently, the HAVEN 6 study has demonstrated the safety and efficacy of emicizumab prophylaxis in moderate/mild hemophilia A patients without inhibitors. In the subgroup of patients with moderate HA and severe bleeding phenotype, a significant reduction of the bleeding rate was observed, leading to the approval of emicizumab prophylaxis in this setting.
Methods: Herein, we report the cases of 3 patients with moderate HA and severe hemorrhagic phenotype, treated with emicizumab prophylaxis and followed at our institution. Patients received emicizumab 3 mg/kg once weekly for 4 weeks, followed by maintenance therapy with 3 mg/kg once every 2 weeks. Data were retrospectively collected from clinical charts.
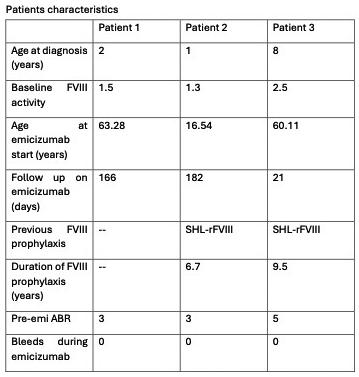
Results: The median baseline FVIII activity (FVIII:C) at diagnosis was 1.5% (range 1.3 - 2.5%). The median age at the time of the first treated bleeding event was 2.01 years (range 0.27 – 2.7 years). First on-demand therapy was represented either by standard half-life recombinant FVIII (SHL-rFVIII) or plasma-derived FVIII concentrate (pdFVIII). Median duration of on-demand therapy was 50.6 years (range 9.9-63.3 years). All 3 patients required switching to a prophylaxis regimen due to frequent breakthrough bleedings; in particular the youngest patient because of very frequent invalidating hematuria and the two other because of frequent spontaneous haemarthroses. Two patients started FVIII prophylaxis at 9.9 and 50.6 years and then were switched to emicizumab for poor compliance to the i.v. infusions and persistence of spontaneous bleeds (after 6.7 and 9.5 years, respectively). A patient transitioned directly from on-demand factor therapy to emicizumab prophylaxis. During FVIII prophylaxis, the median ABR was 3.0 (range 3.0 - 5.0). At the start of emicizumab prophylaxis, the patients had a median age of 60.1 years (range 16.5-63.3) and no-one of them ever had an anti-FVIII inhibitor. At the start of emicizumab prophylaxis, HEAD-US scores were as follows: the youngest patient had a score of 0, while the two older patients—one previously managed with FVIII prophylaxis and the other with on-demand treatment—had scores of 17 and 13, respectively. The median follow-up on emicizumab is 0.5 years (0.1-0.5); during this period, all 3 patients experienced zero bleedings. The two older patients experienced a clinical improvement of hemophilic arthropathy, no longer requiring painkiller medications. The youngest patient experienced a great improvement of his social life, interacting more with his peers, and started to work out at the gym and play basketball.
Conclusions: Despite the small sample size, our experience further supports the efficacy and safety of emicizumab prophylaxis in patients with moderate hemophilia A and a severe bleeding phenotype, even in a real-life setting. Therefore, emicizumab therapy represents a valid alternative to FVIII replacement therapy in this patient population, with some potential advantages in terms of compliance and quality of life.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


