
PO89 | Apixaban for secondary prevention of venous thromboembolism in hemodialysis patients: pharmacokinetic profile and safety outcomes
S. Guglielmo1, E. De Bon2, L. Scarano1, R. Fabris1, E. Pierobon3, S. Barbar2 | 1Internal Medicine, Department of Medicine; 2Thrombotic and Hemorrhagic Disorders Unit, Department of Medicine; 3Nephrology and Dialysis Unit, Azienda ULSS 6 Euganea, Cittadella and Camposampiero, Padua, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background and Aims: The use of direct oral anticoagulants (DOACs) in patients with end-stage renal disease (ESRD) on dialysis remains controversial due to a different pharmacokinetics. To date, dialysis patients have been excluded from all randomized clinical trials and data on these setting are scanty. Among DOACs, apixaban has shown the most favorable profile in this population. We report the case of a female dialysis patient with a history of unprovoked pulmonary embolism and deep vein thrombosis, previously treated with vitamin K antagonists (VKAs), than shifted to apixaban low-dose (2.5 mg twice daily) due to hemorrhagic complications while on VKAs; we focus on apixaban plasma levels and safety outcomes during follow-up.
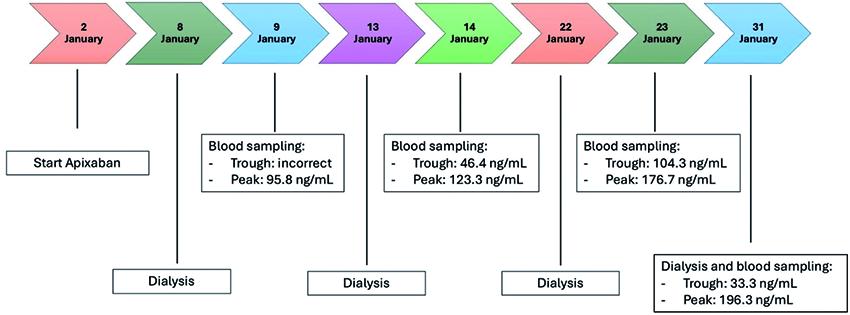
Case Report: We present the clinical course of a 67 year-old female patient with end-stage renal disease undergoing chronic hemodialysis (three times per week), who was treated with apixaban for the secondary prevention of venous thromboembolism. The patient initially received vitamin K antagonists (VKAs) as acute-phase treatment, but this was withheld due to a spontaneous cerebral hemorrhage. She then received thromboprophylaxis with Calciparin, followed by Enoxaparin; both were poorly tolerated due to the route of administration. Apixaban was then started at the dosage of 2.5 mg twice daily. Apixaban plasma concentrations were measured using an anti-Xa assay calibrated specifically for apixaban. Clinical follow-up over six months included monitoring for symptomatic thrombotic events or bleeding complications, and laboratory parameters (i.e. hemoglobin). Apixaban plasma levels measured between day 9 and day 30 of treatment, on four separate occasions - three on non-dialysis days and one on a dialysis day - at both trough and peak times, remained within or slightly above the expected therapeutic range throughout the treatment period, both on dialysis and non-dialysis days. On non-dialysis days, peak concentrations were 95.8, 123.3, and 176.7 ng/mL (reference range: 30–153 ng/mL), while trough concentrations were 46.4 and 104.3 ng/mL (reference range: 11–90 ng/mL), with one trough sample inaccurate. On the dialysis day, peak and trough values were 196.3 ng/mL and 33.3 ng/mL, respectively (Figure 1). No thromboembolic or bleeding complications occurred during follow-up, laboratory values remained stable, and dialysis sessions proceeded without anticoagulation-related issues.
Conclusions: This case supports the potential safety of low-dose apixaban in selected dialysis patients for VTE secondary prevention. In our patient, apixaban levels remained stable within therapeutic ranges, and no adverse events occurred over six months of follow-up. While based on a single case, this report contributes to growing evidence suggesting apixaban may be a viable anticoagulation option in ESRD patients, provided that close clinical and laboratory monitoring is maintained. Larger studies are needed to confirm safety and efficacy in this high-risk population.
Figure 1.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


