
PO37 | Single centre experience on anticoagulation in carriers of non-mild inherited thrombophilia: direct oral anticoagulants (DOAC) efficacy and safety
M. D’uva1,2, G. La Barba1, G. Montanaro1, M. Di Ianni1,2, P. Ranalli1,2 | 1Hematology Unit, S. Spirito Hospital, Pescara; 2Department of Medicine and Aging Sciences, D’Annunzio University, Chieti, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background and Aims: DOAC appear to be a suitable treatment option in patients with inherited thrombophilia (IT), in spite of a few large-scale data on their efficacy in this setting. Rate of venous thromboembolism (VTE) recurrence and bleeding seems to be similar in IT carriers treated with VKA or with DOAC. RIETE Registry showed comparable efficacy and safety of DOAC therapy in subjects with and without IT. Here we report our single centre experience with DOAC use in patients with IT, focusing on non-mild thrombophilia. Our aim consists in the evaluation of DOAC efficacy and safety in this cohort at very high risk of VTE, especially without long term treatment.
Methods: Our single centre retrospective study included n 31 consecutive carriers of non-mild thrombophilia: [protein S deficiency (n 3), protein C deficiency (n 3), ATIII deficiency (n 14) and double heterozygosity FV Leiden + G20210A prothrombin (n 11)] who received diagnosis of deep venous thrombosis (DVT) [n 18], DVT and pulmonary embolism (PE) [n 7] or atypical venous thrombosis [n 5], treated with DOAC. Diagnosis of typical and atypical venous thrombosis and PE were confirmed in all cases by imaging studies (doppler US, CT scan). Clinical data were collected on May 2025 from medical records in our Centre and through telephone calls to the patients. The number of thrombosis recurrence and bleeding events were used as a surrogate of DOAC efficacy and safety respectively.
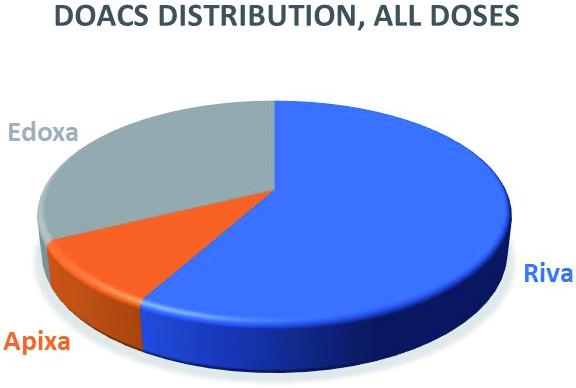
Results: Distribution of DOAC treatments is represented in Figure 1. Among patients treated with rivaroxaban n 13 received full dose (20 or 15 mg OD), n 5 low dose (10 mg OD). All subjects treated with edoxaban received full dose (60 mg OD). All patients who received apixaban were treated with prophylaxis dose (2.5 mg BID). No one received dabigatran. Median time follow-up during DOAC treatment was 74 months (1-120 months). DVT recurrence was observed in a 31 years old female patient (3.2%) with ATIII deficiency receiving rivaroxaban 15 OD, ten years after starting treatment; DVT recurrence occurred concomitantly with the onset of LAC positivity (detected with DOAC remove filter). Therefore warfarin replaced rivaroxaban. Acute Myocardial Infarction (AMI) was diagnosed in a 64 years old male with double heterozygosity FV Leiden + G20210A prothrombin (3.2%) treated with rivaroxaban 15 mg OD after portal vein thrombosis occurred several years before. He did not show cardiovascular risk factors apart from mild hyperhomocysteinemia. After AMI, rivaroxaban was continued, in association with double antiplatelet prophylaxis for six months and then single (aspirin only) until death, two years later due to heart failure. The use of DOAC reduced dose was not associated with thrombosis recurrences. Major hemorrhages were not observed. Moderate bleeding occurred in n 2 patients (6.4%), both triggered by local favoring factors (intraocular and rettorrhagia due to vitreous detachment and IBD respectively). Both patients were receiving DOAC full dose (rivaroxaban and edoxaban respectively). In both cases anemia did not occur, drug dose reduction was not required and bleedings did not leave irreversible marks.
Conclusions: Rivaroxaban, apixaban and edoxaban were efficacious in the high risk population of patients with non-mild IT, also in the long-term observation. Efficacy was confirmed with reduced dose as standard secondary prophylaxis in a subgroup of patients. These agents were safe, as major bleeding did not occur.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


