
PO84 | Beyond the scores: unmasking a silent pulmonary embolism in essential thrombocythemia
N. Battino | ASL Sulcis Iglesiente PO CTO, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background: Pulmonary embolism (PE) is a potentially fatal event, responsible for up to 300,000 deaths annually in Europe. Over 50% of patients with proximal deep vein thrombosis have concurrent PE. The Pulmonary Embolism Severity Index (PESI) and clinical prediction scores such as Wells and Geneva are commonly used for risk stratification. Essential thrombocythemia (ET) is a myeloproliferative neoplasm characterized by clonal thrombocytosis and increased thrombotic and hemorrhagic risk. Severe anemia and extreme thrombocytosis (≥1,000,000/μL) are associated with leukemic transformation. Bone marrow biopsy is key to defining disease stage.
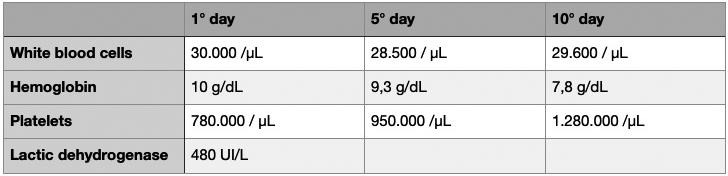
Case Report: A 79-year-old woman with ischemic heart disease and known ET on hydroxyurea (500 mg/day) was admitted for acute respiratory failure and cardiac decompensation. She showed mild tachycardia (110 bpm), tachypnea (25 breaths/min), SpO2 85%, and respiratory alkalosis (pH 7.54). Clinical signs suggested pulmonary congestion. Lab results revealed hemoglobin 10 g/dL, leukocytes 30,000/μL (>80% neutrophils), platelets 780,000/μL, and BNP 572 pg/mL. Echocardiography showed preserved systolic function, moderate mitral/tricuspid insufficiency, and pulmonary artery pressure of 45 mmHg. Despite low Wells and intermediate Geneva scores, the lack of response to therapy prompted further investigation. D-dimer was 1.75 µg/mL. CT pulmonary angiography confirmed segmental acute PE. Doppler ultrasound excluded DVT. Fondaparinux 7.5 mg/day was initiated and later switched to apixaban 5 mg BID, with gradual clinical and respiratory improvement. During hospitalization, hemoglobin declined and platelet count increased (Table 1). No circulating blasts were found on peripheral smear. The patient declined bone marrow biopsy. Genetic testing revealed the JAK2V617F mutation, while BCR-ABL rearrangements were absent.
Conclusions: This case highlights the need to suspect PE in ET patients with respiratory symptoms, even when embolic risk scores are low or intermediate and other diagnoses (e.g., heart failure) are plausible. ET predisposes to thromboembolic complications, particularly in the presence of leukocytosis. Anemia, severe thrombocytosis and new thrombotic-hemorrhagic events concern for possible disease progression. A bone marrow biopsy remains essential when transformation is suspected.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


