PO62 | CLINICAL AND MOLECULAR DIAGNOSTIC CHALLENGES IN MYELOPROLIFERATIVE NEOPLASMS WITH LOW JAK2V617F ALLELIC BURDEN
E. Morsia, D. Lame, M. Pianelli, G. Gramazio, R. Ceccarelli, I. Battilà, S. Rupoli, A. Poloni | Department of Clinical and Molecular Science, Università Politecnica delle Marche, Ancona, Italy

All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background. The detection of the JAK2V617F mutation plays a crucial role in diagnosing myeloproliferative neoplasms (MPNs). In clinical practice, a mutation with a VAF greater than 2% is definitively considered positive, a criterion also used to define Clonal Hematopoiesis of Indeterminate Potential (CHIP). In the MPN field, according to WHO/ICC recommendations, highly sensitive methods should be employed to identify JAK2V617F when the variant allele frequency (VAF) is below 1%. Nevertheless, the assessment of a low JAK2V617F burden remains complex, as this mutation has been observed in individuals without hematological disorders, and no specific cut-off value has been established for MPN diagnosis.
Aims. The aim of this study is to investigate the clinical and molecular features of a cohort of patients who were referred for suspected MPN and who have a JAK2V617F VAF of less than 2%.
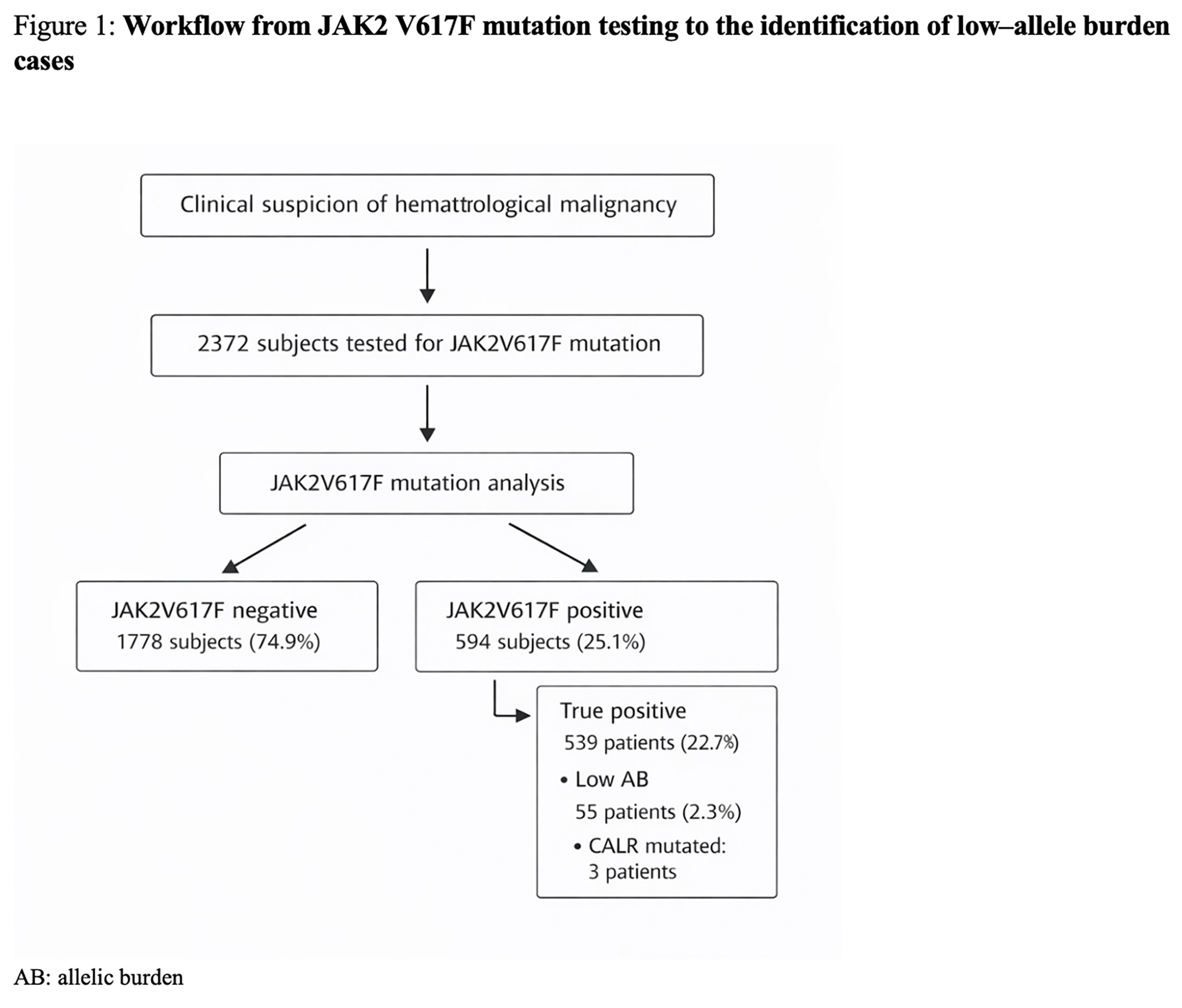
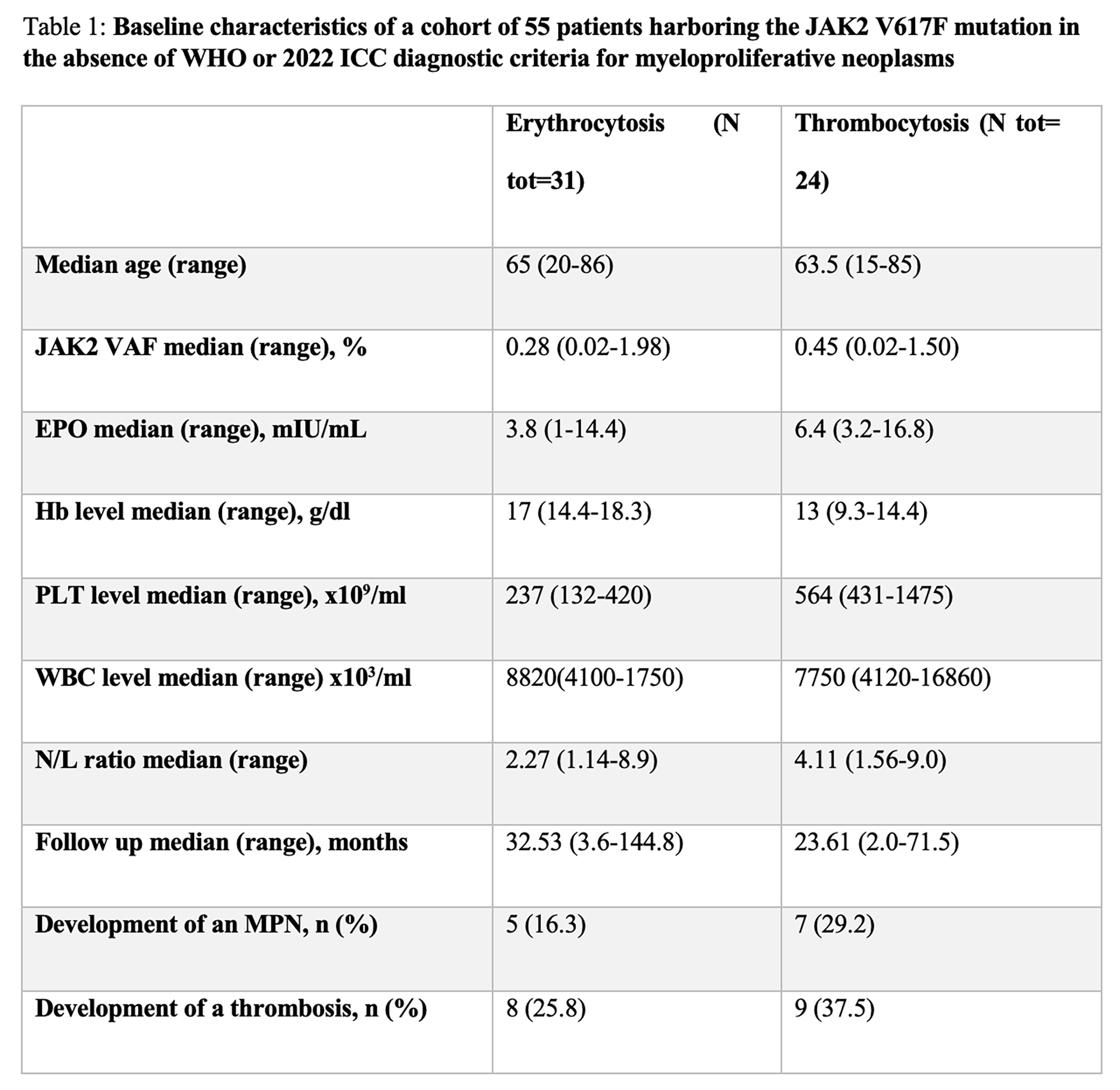
Methods. A total of 55 patients were evaluated at the Hematology Department for erythrocytosis (n=31) or thrombocytosis (n=24) with JAK2V617F VAF < 2%. The study cohort had a median age of 64 years (range: 15–86). JAK2V617F was analyzed in granulocyte samples at the time of diagnostic suspicion using quantitative PCR (ipsogen® JAK2MutaQuant®, LoD 0.0014%).
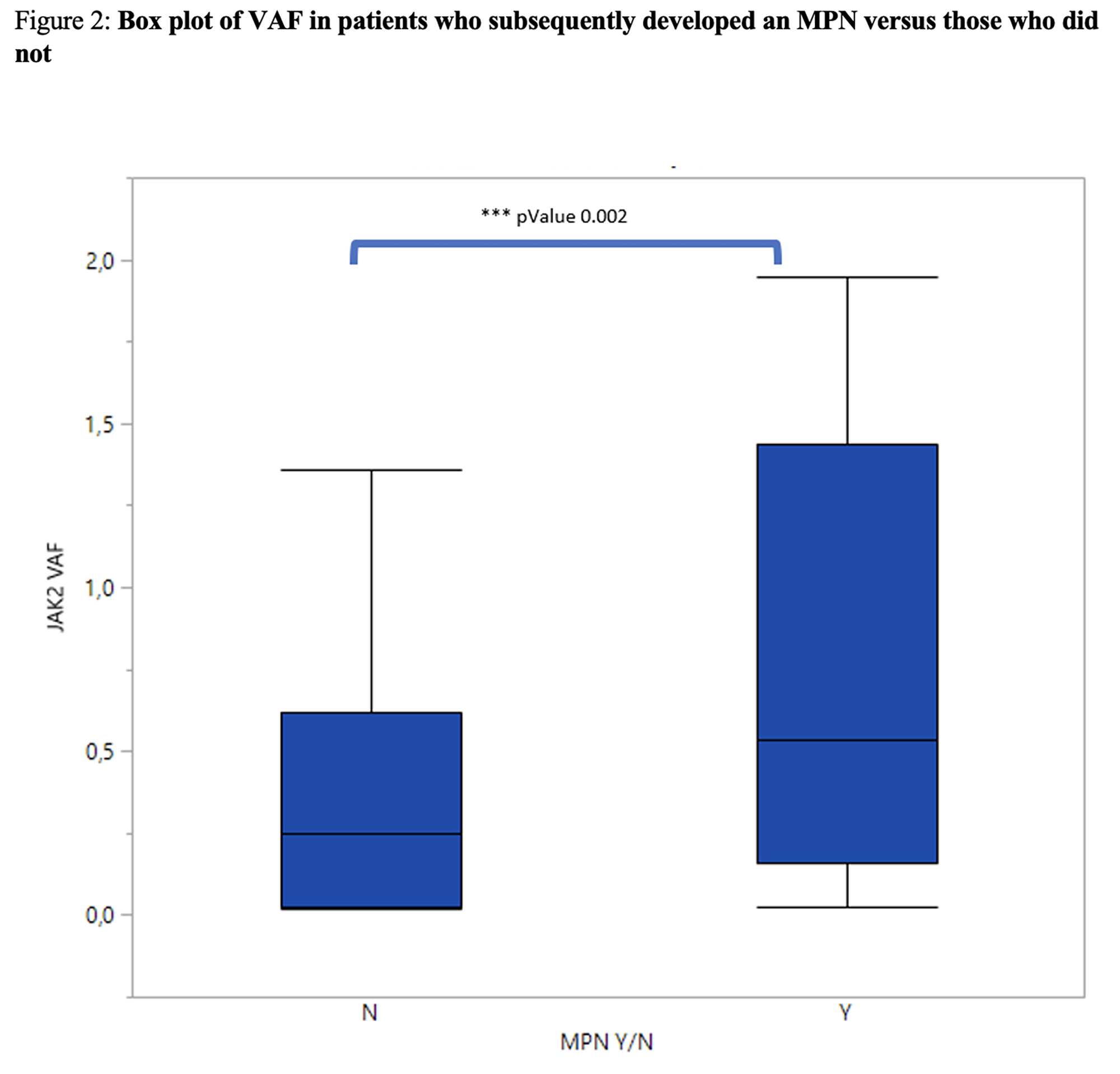
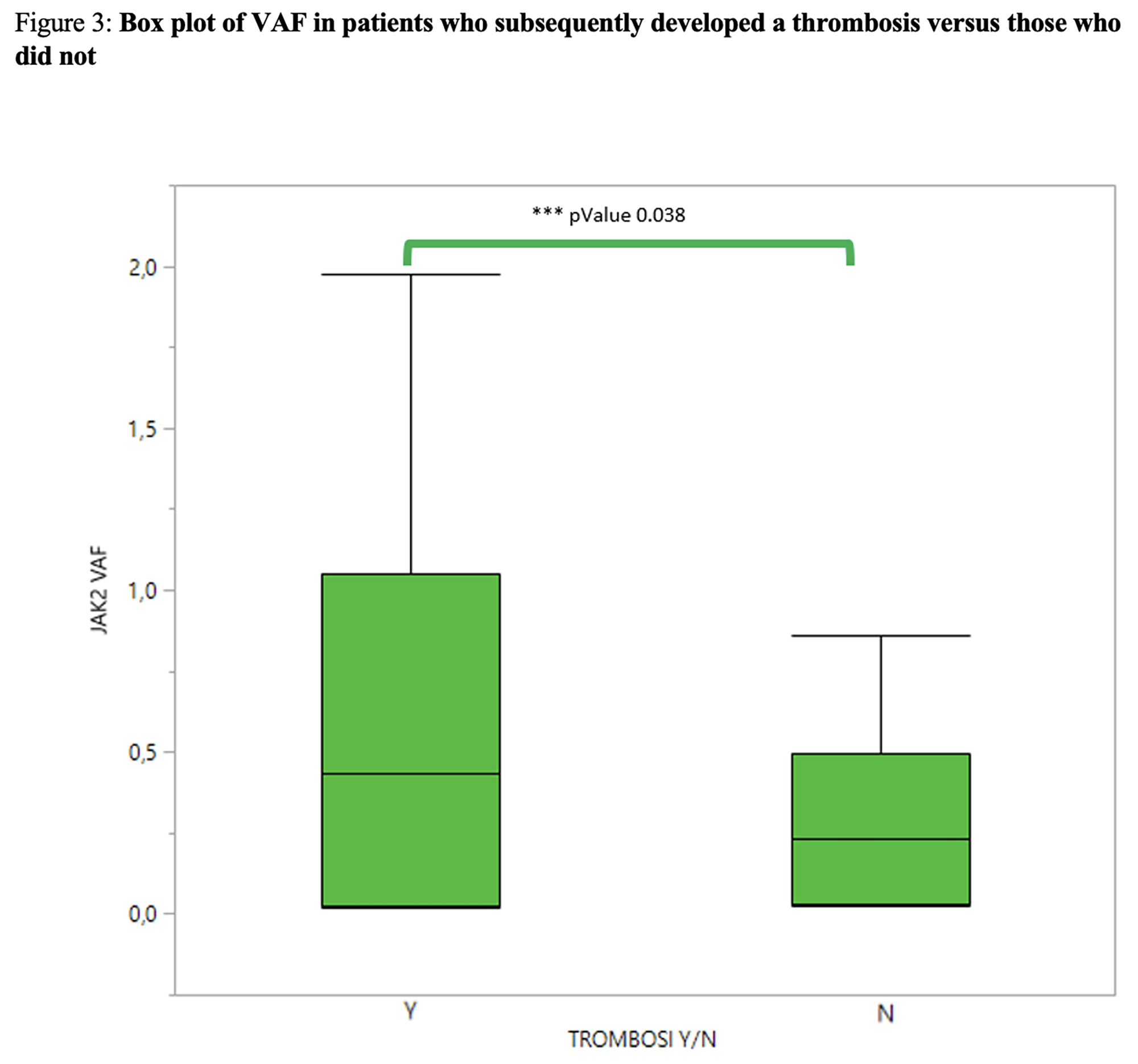
Results. The median JAK2V617F VAF at the time of referral was 0.354% (range: 0.02–1.975), with higher values observed in patients with thrombocytosis compared to those with erythrocytosis (0.451% vs. 0.25%, p=0.047). The median erythropoietin level was 5.4 mU/mL (range: 1–16.8). Among patients with polycythemia, 51% had reduced erythropoietin levels below 5 mU/mL. At the time of the reported quantitative JAK2 test, no patient met the criteria for MPN. Of the 31 cases with erythrocytosis, 4 (12.9%) were ultimately diagnosed with polycythemia vera (PV), and 1 case was diagnosed as pre-fibrotic myelofibrosis (PMF). The median hematocrit was 50.2% (range: 46.2–56.9). Ten cases required phlebotomy, and two patients underwent cytoreductive therapy. Among the 24 cases with thrombocytosis, 7 (22.5%) were diagnosed as essential thrombocythemia (ET). Screening for additional driver mutations identified CALR mutations in three patients with thrombocytosis, all of whom met the criteria for essential thrombocythemia. The median platelet count was 564 × 109/L (range: 451–1475), and 3 out of 24 patients received cytoreductive therapy. The median time from the first quantitative JAK2 assessment to the onset of MPN was 21.06 months (range: 9.2–43.6). When evaluating the VAF at onset, patients who later developed an MPN had a higher median VAF (0.532%, range: 0.023–1.946) compared to those without an MPN diagnosis (0.24%, range: 0.02–1.975; p-value = 0.02). Sequential samples were collected in 27 out of 55 cases, and JAK2V617F was confirmed in all patients. With a median follow-up of 31.7 months, the JAK2V617F clone remained stable over time, with a VAF of less than 2% in all cases. In the studied cohort, 17 patients (30.9%) experienced a thrombotic event, with a median time of 4.34 months from the molecular assessment. Specifically, there were 8 myocardial infarctions, 2 cases of critical limb ischemia, 2 pulmonary embolisms, 2 portal vein thromboses, and 3 lower limb venous thromboses. Among the patients with thrombosis, 52.9% had thrombocytosis. The rate of thrombosis in patients later diagnosed with MPN was comparable to that in those without a diagnosis (25% vs. 32.5%, p-value: 0.57). However, patients who developed thrombosis had a higher median JAK2 allele burden compared to those who did not (0.44% vs. 0.23%, p-value: 0.038).
Conclusions. Comprehensive molecular and clinical characterization of patients with erythrocytosis and/or thrombocytosis and JAK2V617F VAF ≤ 2% led to the diagnosis of MPNs in 21.8% of cases. Patients with low JAK2 allele burden, regardless of MPN diagnosis, appear to have a high thrombotic risk, which correlates with the allele burden of the mutation. Longitudinal studies in this field are needed to enhance diagnostic accuracy and, most importantly, to stratify the thrombotic risk in patients without MPN criteria.

Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Most read articles by the same author(s)
- Società Italiana di Emostasi e Trombosi, PO56 | EXTERNAL VALIDATION OF THE SAVED SCORE IN A CANADIAN REGIONAL CANCER CENTER COHORT: A REAL-WORLD ANALYSIS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO72 | CATHETER-RELATED THROMBOSIS VS. FIBROBLASTIC SLEEVE. INCIDENCE AND IMPACT IN ONCOLOGICAL AND HEMATOLOGICAL PATIENTS WITH PERIPHERALLY INSERTED CENTRAL CATHETER , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, OC04 | DIRECT ORAL ANTICOAGULANTS PROVIDE EFFECTIVE THROMBOPROPHYLAXIS IN NEWLY DIAGNOSED MYELOMA: REAL WORLD FINDINGS FROM THE ATOMM STUDY , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO65 | OVARIC CANCER PRESENTING WITH COLD-AGGLUTININ MEDIATED HEMOLYTIC ANEMIA, PULMONARY THROMBOEMBOLISM AND DEEP VEIN THROMBOSIS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO05 | DESIGN, SYNTHESIS, AND BIOLOGICAL EVALUATION OF NOVEL IMATINIB AND NILOTINIB ANALOGUES EXPRESSING ENHANCED ANTIPLATELET AND ANTICANCER ACTIVITIES , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO55 | HISTORY OF CANCER IN PATIENTS WITH SEVERE HEREDITARY THROMBOPHILIA VERSUS NO THROMBOPHILIA: A SINGLE-CENTER COHORT OF PATIENTS WITH VENOUS THROMBOSIS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO58 | TACKLING THE AWARENESS GAP IN CANCER-ASSOCIATED THROMBOSIS: IMPACT OF A BRIEF EDUCATIONAL INTERVENTION IN PATIENTS WITH GYNECOLOGICAL CANCERS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO60 | VEXAS SYNDROME AS A NEW SEVERE THROMBOPHILIC CLONAL CONDITION: A SINGLE CENTRE EXPERIENCE , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO52 | MECHANISTIC POPULATION PHARMACOKINETIC/PHARMACODYNAMIC AND TIME-TO-EVENT MODELING SUPPORT SUSTAINED FACTOR XI INHIBITION AND SUPERIOR POST-OPERATIVE VENOUS THROMBOEMBOLISM PREVENTION WITH REGN7508CAT , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO68 | RISK OF VENOUS THROMBOEMBOLISM IN PATIENTS WITH CANCER AND MIGRAINE: A COHORT ANALYSIS AMONG DANISH NATIONAL HEALTH SURVEY PARTICIPANTS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)


