PO56 | EXTERNAL VALIDATION OF THE SAVED SCORE IN A CANADIAN REGIONAL CANCER CENTER COHORT: A REAL-WORLD ANALYSIS
A. Naassan, R. Fatima, M. Naassan, C. Chisholm | Lakeridge Health, R.S. McLaughlin Durham Regional Cancer Centre, Department of Oncology, Oshawa, ON, Canada

All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Introduction. Venous thromboembolism (VTE) remains a significant complication in multiple myeloma patients receiving immunomodulatory drugs, with incidence rates of 3-26%. The SAVED score was developed to stratify VTE risk using readily available clinical variables. While initial validation demonstrated strong discriminatory ability in large academic centers, real-world performance in community cancer centers has not been characterized. This study aims to validate the SAVED score in a Canadian Regional Cancer Centre cohort.
Methods. We reviewed 182 multiple myeloma patients who began lenalidomide treatment between January 2013 and February 2025 at the Durham Regional Cancer Centre, with follow-up through January 2026. The SAVED score was calculated using age >80 years (+1), Asian ethnicity (-3), prior VTE (+3), surgery within 90 days (+2), and dexamethasone 120-160 mg monthly (+1) or >160 mg monthly (+2). Patients were classified as low risk (SAVED 0-1) or high risk (≥2). The main result was VTE during lenalidomide therapy, which was confirmed by imaging. Statistical analysis included the Fisher exact test, Kaplan-Meier survival analysis with the log-rank test, and ROC curve analysis. Sensitivity analyses excluded patients with prior VTE and tested alternative cutoffs (≥3).
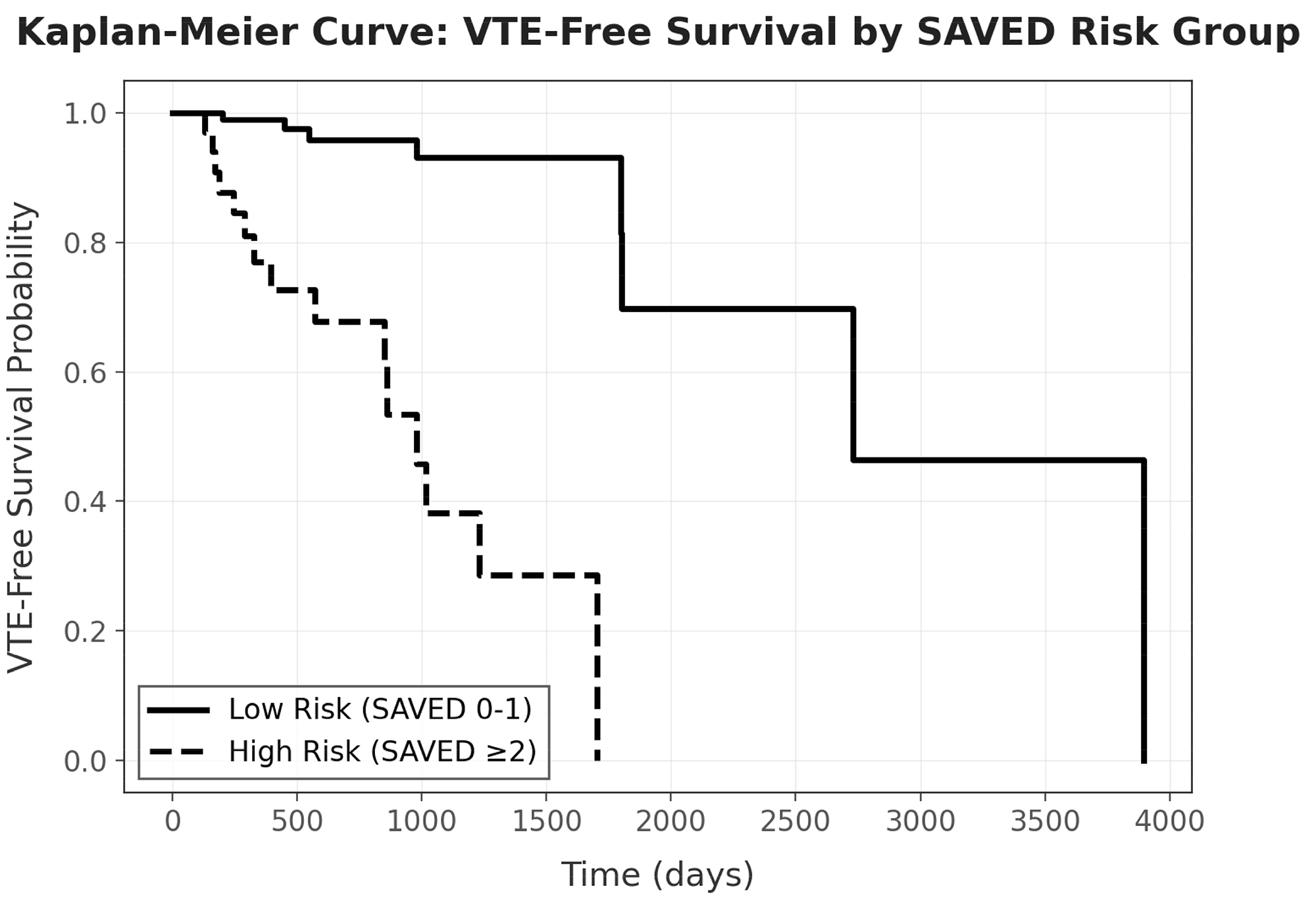
Results. The median age was 79 years. Overall VTE rate was 12.6% (23/182). Low-risk patients (n=139, 76.4%) had a 5.8% VTE rate vs. 34.9% in high-risk patients (n=43, 23.6%). The odds ratio was 8.77 (95% CI 3.39-22.69, p<0.001). The SAVED score showed good discrimination, with an AUC of 0.735 (95% CI 0.611–0.849). Kaplan-Meier analysis showed clear separation (log-rank p<0.001), with median VTE-free survival of 943 days (2.6 years) in high-risk vs 2,703 days (7.4 years) in low-risk patients. Sensitivity analyses confirmed robustness: excluding prior VTE (n=162) yielded OR 8.73 (p<0.001); an alternative cutoff of ≥3 showed OR 6.88 (p<0.001).
Conclusions. The SAVED score successfully stratified VTE risk in our community cancer center cohort, with high-risk patients demonstrating a 9-fold increased odds of VTE and significantly shorter VTE-free survival. These results support SAVED score-guided thromboprophylaxis decisions in community practice settings where most myeloma patients receive care. Future work should focus on evaluating the impact of SAVED score-guided thromboprophylaxis on VTE reduction and the cost-effectiveness of risk-stratified approaches to thromboprophylaxis in the community cancer center setting.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Most read articles by the same author(s)
- ICTHIC 2026, OC04 | DIRECT ORAL ANTICOAGULANTS PROVIDE EFFECTIVE THROMBOPROPHYLAXIS IN NEWLY DIAGNOSED MYELOMA: REAL WORLD FINDINGS FROM THE ATOMM STUDY , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- ICTHIC 2026, PO61 | RISK FACTORS FOR INTRACRANIAL HEMORRHAGE: AN UMBRELLA REVIEW TO INFORM MACHINE LEARNING PREDICTION MODELS IN GLIOMA PATIENTS RECEIVING ANTICOAGULATION , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- ICTHIC 2026, PO72 | CATHETER-RELATED THROMBOSIS VS. FIBROBLASTIC SLEEVE. INCIDENCE AND IMPACT IN ONCOLOGICAL AND HEMATOLOGICAL PATIENTS WITH PERIPHERALLY INSERTED CENTRAL CATHETER , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- ICTHIC 2026, PO55 | HISTORY OF CANCER IN PATIENTS WITH SEVERE HEREDITARY THROMBOPHILIA VERSUS NO THROMBOPHILIA: A SINGLE-CENTER COHORT OF PATIENTS WITH VENOUS THROMBOSIS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- ICTHIC 2026, PO65 | OVARIC CANCER PRESENTING WITH COLD-AGGLUTININ MEDIATED HEMOLYTIC ANEMIA, PULMONARY THROMBOEMBOLISM AND DEEP VEIN THROMBOSIS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- ICTHIC 2026, PO62 | CLINICAL AND MOLECULAR DIAGNOSTIC CHALLENGES IN MYELOPROLIFERATIVE NEOPLASMS WITH LOW JAK2V617F ALLELIC BURDEN , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- ICTHIC 2026, PO05 | DESIGN, SYNTHESIS, AND BIOLOGICAL EVALUATION OF NOVEL IMATINIB AND NILOTINIB ANALOGUES EXPRESSING ENHANCED ANTIPLATELET AND ANTICANCER ACTIVITIES , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- ICTHIC 2026, PO52 | MECHANISTIC POPULATION PHARMACOKINETIC/PHARMACODYNAMIC AND TIME-TO-EVENT MODELING SUPPORT SUSTAINED FACTOR XI INHIBITION AND SUPERIOR POST-OPERATIVE VENOUS THROMBOEMBOLISM PREVENTION WITH REGN7508CAT , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- ICTHIC 2026, PO68 | RISK OF VENOUS THROMBOEMBOLISM IN PATIENTS WITH CANCER AND MIGRAINE: A COHORT ANALYSIS AMONG DANISH NATIONAL HEALTH SURVEY PARTICIPANTS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- ICTHIC 2026, PO50 | SUB-ANALYSIS OF INTERIM RESULTS FROM A PHASE 2 STUDY INVESTIGATING REGN9933A2 AND REGN7508CAT FOR THE PREVENTION OF CONTACT-MEDIATED VENOUS THROMBOEMBOLISM IN PATIENTS WITH ACTIVE CANCER UNDERGOING PERIPHERALLY INSERTED CENTRAL CATHETER PLACEMENT (ROXI-CATH) , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)


