PO28 | CLINICAL IMPLICATIONS OF ANTICOAGULANT DRUG INTERACTIONS WITH TARGETED AND IMMUNE THERAPIES IN ONCOLOGY: A CONTEMPORARY RISK STRATIFICATION FRAMEWORK
D. Dhami1, C. Solowiej Singh 1, M. Dhami 2 | 1Abrazo Internal Medicine Residency; 2Eastern Connecticut Hematology Oncology, Norwich, CT, USA

All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background. Anticoagulation in patients with cancer is challenging due to competing risks of thrombosis and bleeding. The expanding use of targeted therapies and immune checkpoint inhibitors further complicates management, as many agents interact with commonly used anticoagulants. Recent guidance from the American Society of Clinical Oncology and American Heart Association along with emerging registry and pharmacokinetic data, provides an opportunity to refine anticoagulation strategies in this population.
Aims. This review evaluates drug–drug interactions (DDIs) between anticoagulants and cancer-directed therapies using pharmacokinetic, clinical, and registry data. We propose a practical, risk-based framework to guide anticoagulant selection.
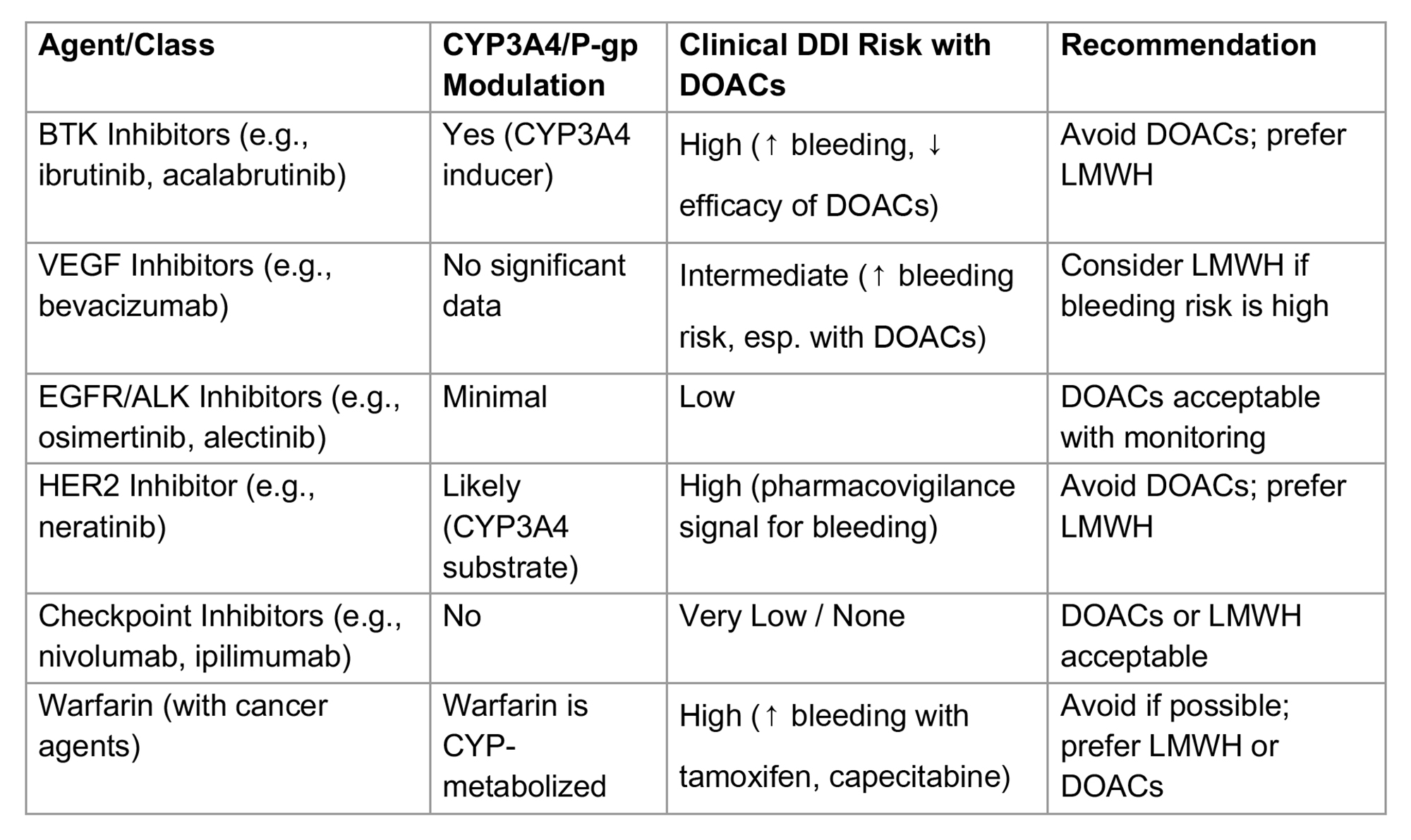
Methods. We reviewed registry studies, systematic reviews, expert consensus guidelines, and pharmacologic data addressing DDIs between anticoagulants and cancer therapies. Interaction risk was categorized and incorporated into a clinical framework for selecting direct oral anticoagulants (DOACs), low molecular weight heparin (LMWH), or vitamin K antagonists (VKAs) in patients receiving VEGF, BTK, EGFR, ALK, HER2, and immune checkpoint inhibitors.
Results. Targeted therapies demonstrate variable DDI profiles with DOACs, largely mediated by CYP3A4 and P-glycoprotein pathways. BTK inhibitors, particularly ibrutinib, are associated with increased bleeding risk due to combined pharmacokinetic, antiplatelet, and arrhythmogenic effects. VEGF inhibitors also confer elevated bleeding risk when combined with certain DOACs. In contrast, most immune checkpoint inhibitors lack clinically significant pharmacokinetic DDIs, though immune-mediated toxicities may contribute to bleeding. A structured classification system was developed to guide anticoagulant selection. LMWH is preferred in patients receiving strong CYP3A4/P-gp modulators or with GI/GU malignancies, while VKAs are often deprioritized due to unpredictable effects. Registry data suggest bleeding events exceed recurrent thrombosis in select high-risk pairings.
Conclusions. We present a clinically actionable framework for anticoagulation management in cancer patients receiving targeted and immune therapies. Risk-based anticoagulant selection, informed by pharmacologic and clinical data, can reduce adverse events while maintaining efficacy.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Most read articles by the same author(s)
- Società Italiana di Emostasi e Trombosi, PO02 | SYNERGISTIC INTERACTION OF ENDOTHELIAL AND CANCER CELLS IN THE FORMATION AND STRUCTURE OF THE FIBRIN CLOT SHIELDS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, OC11 | COMPLEXITIES IN MANAGING ANTITHROMBOTIC THERAPY IN PATIENTS WITH CANCER APPROACHING END-OF-LIFE: A MIXED METHOD INTEGRATION USING JOINT DISPLAY ANALYSIS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO37 | CLINICAL SIGNIFICANCE OF SYMPTOMATIC AND INCIDENTAL VENOUS THROMBOEMBOLISM IN CANCER PATIENTS TREATED WITH APIXABAN , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, OC12 | RISK OF VENOUS THROMBOEMBOLISM AFTER REMOVAL OF AN UPPER EXTREMITY CENTRAL CATHETER ASSOCIATED WITH A DEEP VEIN THROMBOSIS IN CANCER PATIENTS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO04 | FIBRIN CLOT SHIELDS PROMOTE CLONAL SELECTION IN CANCER CELLS: PROCOAGULANT ACTIVITY AND SURVIVAL OF CLOT-EMBEDDED CELLS. A NOVEL TUMOR MICROENVIRONMENT MODEL , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO22 | LONG-TERM ANTICOAGULANT THERAPY AND REDUCTION OF OVARIAN CANCER RECURRENCE: CLINICAL EVIDENCE OF A POTENTIAL ANTITUMOUR EFFECT , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO07 | PLATELET INHIBITION BY THE NOVEL NITRIC OXIDE-DONOR NITROSOOXYPROPANOL , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO13 | OUTPATIENT TREATMENT OF VENOUS THROMBOEMBOLISM AND SUBSEQUENT RISK OF CANCER , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO17 | PREDICTIVE VALUE OF INFLAMMATORY AND ENDOTHELIAL BIOMARKERS FOR CANCER RISK IN HEALTHY INDIVIDUALS: EVIDENCE FROM THE HYPERCAN STUDY , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, OC08 | A SILK-BASED 3D BONE MARROW MODEL FOR CHEMOTHERAPY-INDUCED THROMBOCYTOPENIA , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)


