OC05 | TIME TO START OF ANTICOAGULANT THERAPY AND SURVIVAL OUTCOMES IN CANCER PATIENTS WITH PULMONARY EMBOLISM
K. Bria, B. Gage, M. Bealsey, K. Sanfilippo | Washington University in St. Louis School of Medicine, St. Louis, MO, USA

All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Introduction. Pulmonary embolism (PE) is a leading cause of death in cancer. Those with cancer-associated thrombosis have mortality rates 2–5x higher than other cancer patients. Prior data shows that therapeutic anticoagulant therapy (AT) within 24 hours of PE diagnosis can reduce mortality.
Aim. We aimed to evaluate 30-day PE-associated mortality and time to start AT in patients with and without active cancer.
Methods. We performed a retrospective cohort study of patients who presented to the emergency room at Barnes Jewish Hospital with symptoms of PE between 1/2021 and 12/2025. Only patients initiated on AT with unfractionated or low-molecular-weight heparin and diagnosed with intermediate- or high-risk PE were included. We identified patients who died within 30 days from a PE-related cause and compared mortality rates in those with and without active cancer. We also compared the time from patient presentation (triage vital signs) to PE diagnosis (on objectively confirmed imaging studies), from PE diagnosis to the start of AT, and from patient presentation to the start of AT.
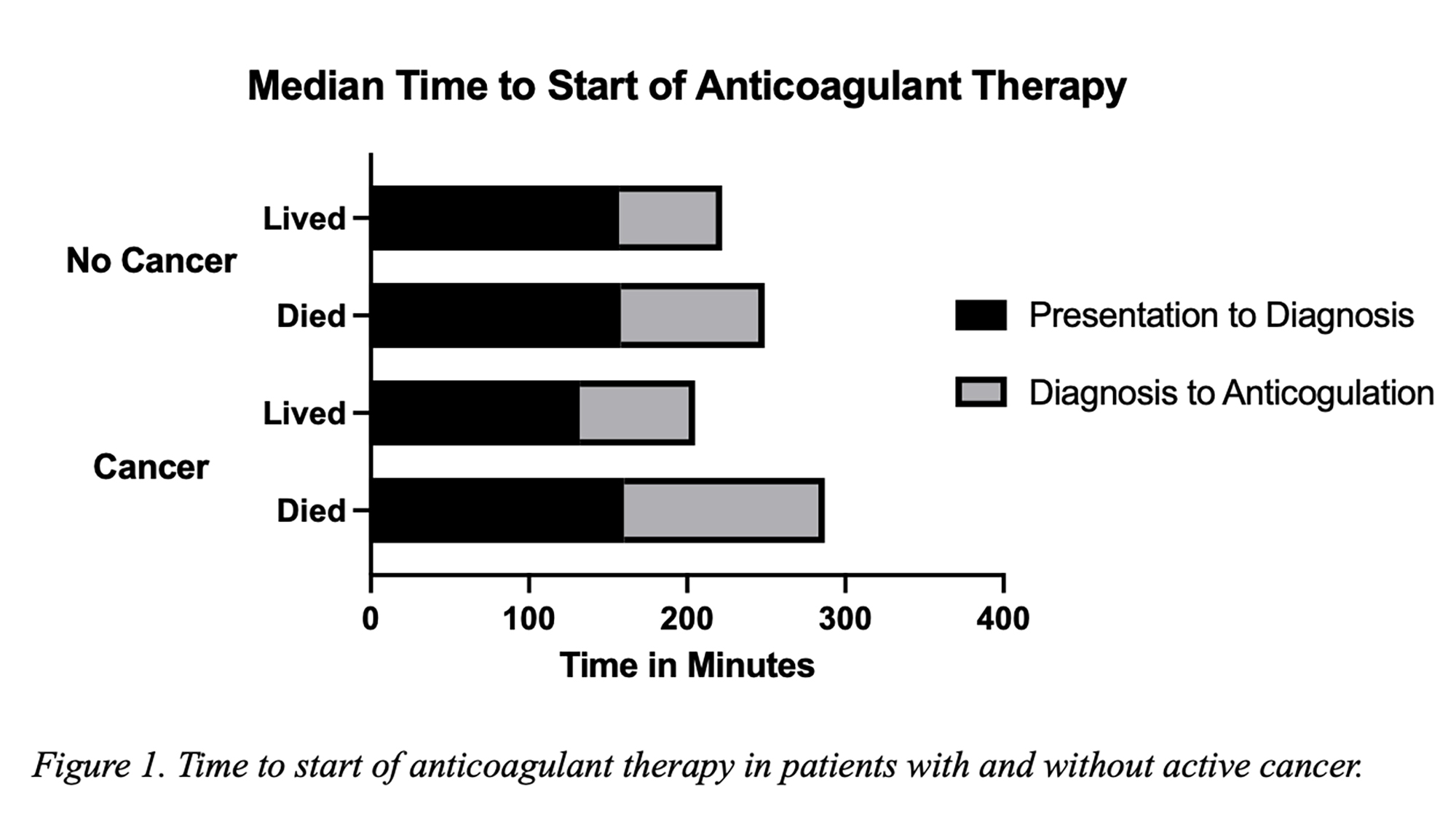
Results. 400 patients met inclusion criteria: 102 patients with active cancer and 298 patients without. Among the patients with cancer, 15 (13.7%) experienced 30-day PE-associated mortality compared to 21 (7.0%) of patients without cancer. The median time to start AT was shorter among patients without cancer (231 minutes) compared to those with cancer (273 minutes) and those who lived (232 minutes) compared to those who died (254 minutes). Among cancer patients, the median time to the start of AT was 259 minutes in patients who lived vs. 304 minutes in those who died. Patients with cancer were diagnosed more quickly with PE (137 minutes) compared to those without (158 minutes). However, they experienced longer delays from PE diagnosis to AT initiation: 75 minutes (cancer) vs. 66 minutes (no cancer). Patients with cancer were more likely to be of older age (69.5 years vs. 62 years), have a lower eGFR (70.5/min vs. 87.8 mL/min), and be thrombocytopenic (30.3% vs. 14.1%).
Conclusions. In patients with intermediate- or high-risk PE, those with active cancer died from a PE-related cause at nearly twice the rate of those without cancer. Despite being diagnosed with PE more quickly, patients with cancer had longer delays in AT initiation, possibly related to comorbidities (i.e., older age, lower eGFR, and thrombocytopenia). Further studies are needed to investigate the optimization of time to AT initiation.

Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Most read articles by the same author(s)
- Società Italiana di Emostasi e Trombosi, PO24 | WE ARE JUGGLING MANY POSSIBILITIES: HEALTHCARE PROFESSIONALS’ EXPERIENCES AND PERSPECTIVES ON INTERPRETATION OF PULMONARY EMBOLISM SIGNS AND SYMPTOMS IN PATIENTS WITH LUNG CANCER , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO19 | THE INTER-RELATIONSHIP BETWEEN NETOSIS, THE ADAMTS-13/VWF AXIS, AND HEMOSTATIC ACTIVATION IN PATIENTS WITH GYNECOLOGICAL MALIGNANCIES: PROGNOSTIC SIGNIFICANCE AND IMPACT OF CHEMOTHERAPY , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO69 | INCIDENTAL CANCER DETECTED DURING EMERGENCY DIAGNOSTIC WORK-UP FOR ACUTE PULMONARY EMBOLISM: A RETROSPECTIVE COHORT STUDY , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO20 | DYSFUNCTION OF THE ADAMTS-13/VON WILLEBRAND FACTOR AXIS, MEDIATED BY NETOSIS, AS A DRIVER OF PROTHROMBOTIC STATE AND UNFAVORABLE PROGNOSIS IN ONCOGYNECOLOGICAL PATIENTS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO44 | PREDICTORS OF ONE-YEAR MORTALITY IN NEWLY DIAGNOSED METASTATIC BREAST CANCER: THE PROGNOSTIC ROLE OF HEMOSTATIC BIOMARKERS AND EARLY THROMBOEMBOLISM , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO21 | PSYCHOLOGICAL IMPACT OF CANCER-ASSOCIATED THROMBOSIS: DUAL BURDEN AND IMPLICATIONS FOR QUALITY OF LIFE AND INTEGRATED PATIENT-CENTERED CARE , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, OC13 | VON WILLEBRAND FACTOR PREDICTS POOR OUTCOME IN PANCREATIC CANCER AND MEDIATES TUMOR-ENDOTHELIUM INTERACTIONS FACILITATING METASTASIS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO09 | CANCER MORTALITY AFTER INCIDENT VENOUS THROMBOEMBOLISM , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO29 | CANADIAN INSIGHTS INTO THE MANAGEMENT OF BREAKTHROUGH THROMBOSIS , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)
- Società Italiana di Emostasi e Trombosi, PO38 | PERICATHETER AND SYSTEMIC THROMBOSIS DURING CAR-T LYMPHOCYTAPHERESIS: INCIDENCE AND CLINICAL CORRELATES , Bleeding, Thrombosis and Vascular Biology: Vol. 5 No. s1 (2026)


