
CO50 | Diagnostic accuracy of the heparin-induced multiple electrode aggregometry (HIMEA) functional test for heparin-induced thrombocytopenia
M. Bovara1, M. Sebastiani2, Am. Gori3,4, A. Rogolino3,4, A. Bertelli3,4, G. Ciarrocca Taranta3,4, R. Marcucci3,4, M. Sartori5, B. Cosmi5, M. Silingardi6, A. M. Pizzini6, A. Marrocchi1, R. Mancini1 | 1Laboratorio Unico Metropolitano Ospedale Maggiore, AUSL Bologna; 2IRCCS Istituto delle Scienze Neurologiche, Bologna; 3Centro Malattie Aterotrombotiche Azienda Ospedaliera Universitaria Careggi, Firenze; 4Dipartimento di Medicina Sperimentale e Clinica, Università di Firenze; 5U.O. di Angiologia e Malattie della Coagulazione dell’Azienda Ospedaliero Universitaria Policlinico S. Orsola-Malpighi, Bologna; 6Medicina Interna Ospedale Maggiore, Bologna, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background and Aims: Heparin-Induced Thrombocytopenia (HIT) is a clinical syndrome that may cause thrombotic complications in patients receiving heparin therapy. The 4T score assesses pre-test probability: if intermediate or high, an immunological test is required to detect anti-heparin/PF4 antibodies. A negative result excludes HIT, while a positive test requires functional confirmation, as some patients have non-pathogenic antibodies. Functional HIT tests identify clinically relevant antibodies, but gold-standard methods such as Heparin-Induced Platelet Aggregation (HIPA) require washed platelets and specialized expertise, limiting access. The Heparin-Induced Multiple Electrode Aggregometry (HIMEA) test, which uses whole blood as platelet source, is simpler and may serve as a valid alternative. This study evaluates HIMEA’s performance for implementation in the workflow at the Metropolitan Unified Lab (LUM) in Bologna, comparing sensitivity and specificity with the HIPA assay conducted at a specialized center.
Methods: Between 2019 and 2025, serum from 78 HIT-positive patients based on the HIT immunological test using chemiluminescence (Hemosil HIT, Werfen Spa) were stored at -80°C at LUM. In 2024-2025, these samples underwent functional HIMEA testing using the Multiplate aggregometer. The HIMEA test was conducted using patient serum, whole blood in hirudin-containing tubes from donors responsive to HIT antibodies, selected using the monoclonal antibody 5B9 (Stagò Spa), and low/high doses of unfractionated heparin (UH, 1 and 200 U/mL). To evaluate HIMEA performance, 54 of the 78 serum samples were also analyzed using the HIPA method at the Atherothrombotic Diseases Laboratory of AOSP Careggi. The HIPA assay utilizes patient serum, washed platelets from 5 donors, and UH (0.2 and 100 U/mL). ROC analysis determined the optimal cut-off and diagnostic accuracy of the HIMEA method was evaluated in comparison to HIPA.
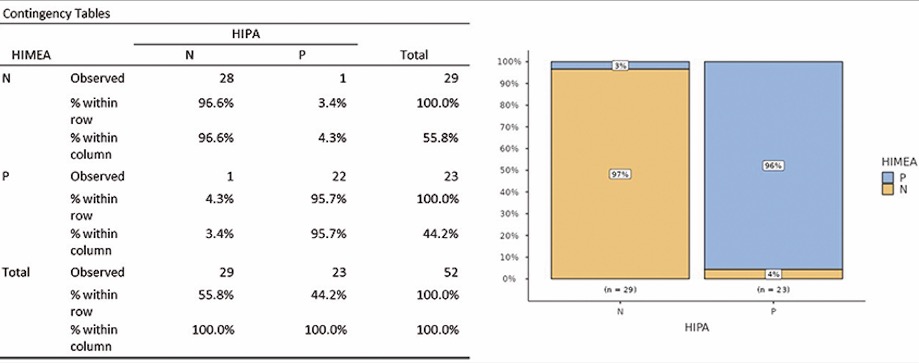
Results: HIMEA classified 42% of samples as positive (n=33), 53% as negative (n=41), and 5% as inconclusive (n=4). The high negative rate confirms the need for functional HIT testing to avoid misclassification. To assess diagnostic accuracy, 54 samples were also analyzed using HIPA; two inconclusive HIMEA results were excluded. ROC curve identified an optimal cut-off of 34 U, yielding 96.9% sensitivity, 90.5% specificity. The HIMEA test demonstrated a positive predictive value (PPV) of 95.7% and a negative predictive value (NPV) of 96.6% when compared to the HIPA assay. Two discordant cases emerged: one false negative due to poor platelet donor responsiveness and one false positive without a clear explanation.
Conclusions: Among the 78 patients who tested positive for the HIT immunological test in the Bologna area, 53% were negative with HIMEA test. The immunological HIT assay has high sensitivity but lower specificity, making functional tests fundamental for completing the HIT diagnostic algorithm and preventing misclassification based solely on immunological testing. The comparison between the HIMEA test and the HIPA assay performed at a specialized reference center suggests that HIMEA may be a reliable diagnostic tool with promising sensitivity and specificity, supporting its implementation at LUM. A critical limitation remains the occurrence of inconclusive results, which may limit clinical applicability. Further validation in real-world settings is warranted to better define its role in routine practice.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


