
CO47 | Genetic characterization of the KIV2 LPA polymorphism in subjects with bicuspid aortic valve with different clinical complications
R. Orsi1, G. Barbieri1, E. Sticchi1,2, A. Kura1, L. Squillantini1, P. Cantini1, A. Rogolino2, M. Berteotti1,2, S. Nistri3, P. Stefàno4, R. Marcucci1,2, B. Giusti1,2 | 1Department of Experimental and Clinical Medicine, University of Firenze; 2Centre for Atherothrombotic Diseases, AOU Careggi, Firenze; 3Cardiology, CMSR Veneto Medica, Altavilla Vicentina; 4Cardiac Surgery, AOU-Careggi, Firenze, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background and Aims: The bicuspid aortic valve (BAV) is the most common congenital cardiopathy affecting 0.5 to 2.0% of the general population. This condition can cause secondary complications such as valvular aortic stenosis, calcification, aortic insufficiency and thoracic aortic aneurysm. Beyond hemodynamic valvular impairment, a frequent determinant of BAV natural history, dyslipidemia and elevated lipoprotein (a) [Lp(a)] levels also favour progression and complications of BAV disease. Lp(a) levels are known to be under a strict genetic control (heritability of the trait >90%) and are largely influenced by LPA Kringle IV type 2 (KIV2) size polymorphism: a lower number of KIV2 repeats is associated with higher levels of circulating Lp(a). In this study, we characterized LPA KIV2 repeats, using a digital droplet PCR (ddPCR) approach, in a cohort of BAV patients with different clinical settings.
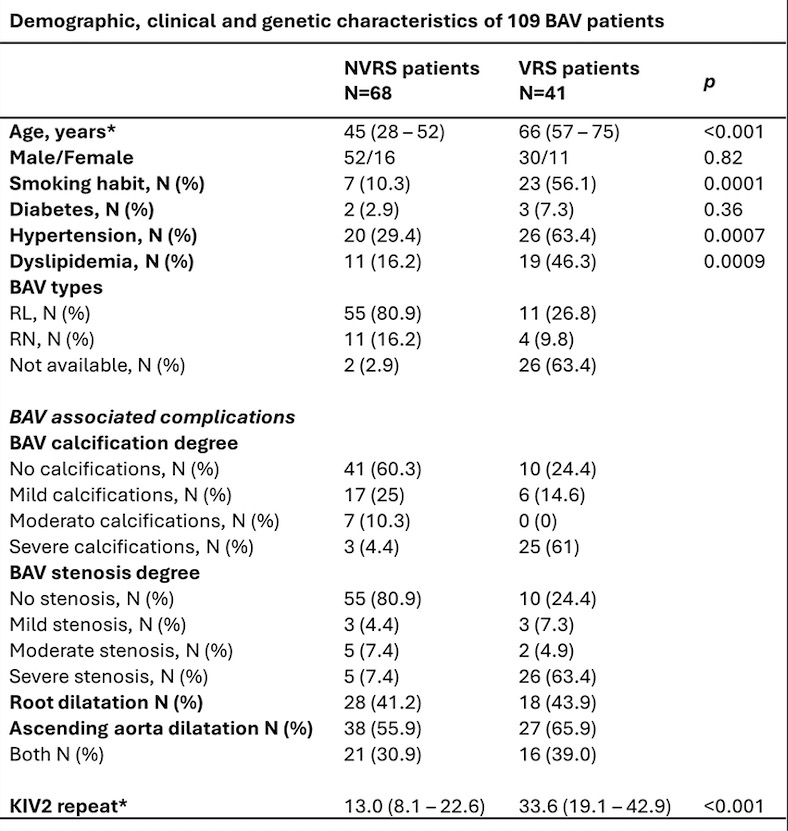
Methods: One hundred nine subjects of Caucasian origin referred to the Regional Referral Center for Marfan syndrome and related disorders and to the Advanced Molecular Genetics Laboratory (Atherothrombotic Diseases Center, AOU-Careggi) were enrolled. Patients were divided into two groups according to different clinical settings: 1) patients undergoing valve replacement surgery (VRS, n=68 subjects) and 2) patients not undergoing valve replacement surgery (NVRS, n=41 subjects). The genetic characterization of the LPA KIV2 polymorphism was carried out through ddPCR (Bio-Rad).
Results: NVRS and VRS patients showed, respectively, significant differences in median age (IQR) [45 (28-52) vs. 66 (57–75), p<0.001], and in classical cardiovascular risk factors such as dyslipidaemia [11 (16.2%) vs. 19 (46.3%), p=0.0009], hypertension [20 (29.4%) vs. 26 (63.4%), p=0.0007], and smoking habit [7 (10.3%) vs. 23 (56.1%), p=0.0001], as expected. The prevalences of aortic stenosis, calcification and aortic root/thoracic ascending aorta dilatation, according to different severity degree in both groups, are reported in the enclosed Table 1.We also observed a significant difference in the median number of KIV2 repeats between the two groups [13 (8.1 – 22.6) in NVRS vs. 33.6 (19.1 – 42.9) in VRS, p<0.001]. As concerns KIV2 repeat evaluation according to BAV clinical complications, NVRS patients with complications showed a trend towards reduction in the number of KIV2 repeats with respect to NVRS patients without complications [stenosis: 10,90 (7.1 – 19.9) vs. 13.21 (9.2 – 24.4), p=0.341; calcification: 12.6 (7.2 – 20.3) vs. 15 (9.88 – 24.5), p=0.319; root dilatation: 11.9 (6.9 – 18.6) vs. 15.8 (10.4 – 24.0), p=0.165]. Moreover, we observed a statistically significant decrease in KIV2 repeats number in NVRS patients with thoracic ascending aorta dilatation with respect to those without dilatation [11.2 (6.7 – 17.6) vs. 18.8 (11.8 – 25.9), p=0.016]. In VRS patients, instead, no significant difference in the distribution of the number of KIV2 repeats, according to the presence or absence of BAV clinical complications, was found.
Conclusions: Our analysis suggests that in NVRS patients, younger and with a lower prevalence of traditional cardiovascular risk factors than VRS ones, higher levels of genetically determined lipoprotein (a) might contribute to the development of BAV complications and in turn to a worse prognosis. Data observed in VRS patients might be likely due to the not negligible impact of cardiovascular risk factors burden in influencing the phenotype severity.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


