
CO45 | Role of urinary 11-dehydro-thromboxane B2 as a predictor of preeclampsia in pregnant high-risk women on low-dose aspirin treatment
P.G.M. Simeone1, R. Liani1, M. Alfonsetti1, A. Ricci1, V. Cianci1, S. Zeeba2, M. Molino3, S. Palma2, R. Malizia4, M. Luongo4, A. Di Castelnuovo5, F. Cipollone1, F. D’antonio6, F. Ricci2, G. Renda2, F. Santilli1 | 1Department of Medicine and Aging Sciences, Center for Advanced Studies and Technology, University of Chieti; 2Department of Neuroscience, Imaging and Clinical Sciences, G D’Annunzio University of Chieti-Pescara, Chieti; University Cardiology Division, Heart Department, Policlinico SS Annunziata, Chieti; 3Clinical Pathology of Chieti University Hospital; 4Immunotransfusion Service, Clinical Haematology of Chieti University Hospital, Chieti; 5Mediterranea Cardiocentro, Napoli; 6Centre for Fetal Care and High-Risk Pregnancy, Department of Obstetrics and Gynecology, University of Chieti, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background and Aims: Pre-eclampsia (PE) is the leading cause of adverse cardiovascular (CV) outcomes during and after pregnancy. Thromboxane (TX)-dependent platelet activation plays a key role in PE pathogenesis. Urinary 11-dehydro-TXB2, a major TX metabolite (TXM), is reduced by at least 75% by low-dose aspirin (ASA) treatment and predicts the occurrence of CV events and mortality in individuals with and without CV disease on ASA. Low-dose ASA showed to effectively prevent PE, even though an interindividual variability in ASA responsiveness exists. Our aims were to identify platelet and circulating biomarkers and clinical predictors of PE in patients at high risk for PE.
Methods: We enrolled 24 women with pregnancy at high risk for PE and 11 women with physiological pregnancy in an ongoing study. At first visit and every trimester, women underwent clinical evaluation, CV imaging, blood and urine sampling for biochemical markers of platelet activation. Based on the slope of sTXB2 between 10 and 24 hours after ASA intake, which indicates the recovery rate of COX-1 activity, women at risk for PE were stratified into tertiles.
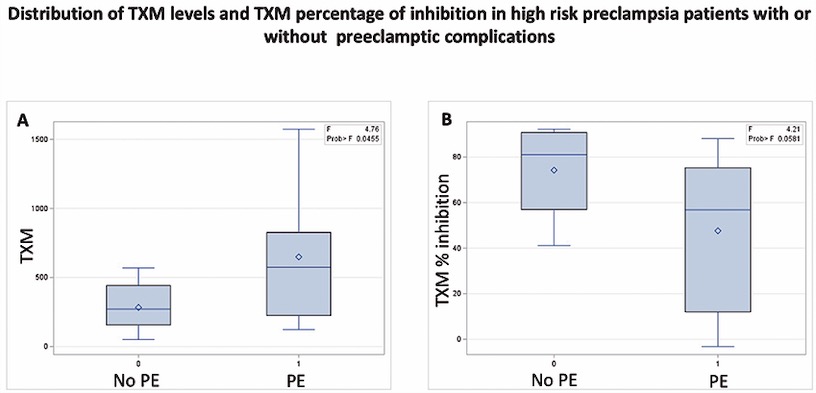
Results: At baseline, the two groups did not differ in parameters except for higher glucose and cholesterol levels, lower PAPP-A and PLGF in pregnancies with high PE risk. TXM and circulating P-selectin were not different between groups at baseline, while, as expected, were significantly reduced during ASA treatment compared to healthy women, consistent with the predominant platelet source of TXM. Higher levels of TXM during the II trimester characterized women at high PE risk with serumTXB2 slope in the third vs. I tertile. Six patients at high PE risk experienced childbirth with PE. Compared to high PE risk women who did not develop events (no PE), women who developed PE were more hypertensive (p=0.01), had higher basal body weight (p=0.056), family history of coronary artery disease (p=0.031), lymphocyte count, C-reactive protein (CRP) [I, p=0.028 and III trimester, p=0.042)], higher percentage of immature platelets, higher urinary TXM (p=0.020) and a higher percentage of platelet P-selectin (p=0.072) in the II trimester. Interestingly, patients who developed PE had a suboptimal, lower than 75% TXM percent inhibition (p=0.058) during II trimester of pregnancy (mean 57% vs. 87%, Figure 1 B). Women with TXM<75% have an odds ratio 2.40 (95% CI: 0.30 to 19.04; P=0.41) of developing PE. Finally, TXM during II trimester, adjusted for baseline values, predicted the development of PE despite ASA, among at-risk patients (p=0.035).
Conclusions: Residual, TX-dependent platelet activation is associated with a shorter duration of ASA effect over the 24-hour dosing interval and may predict the occurrence of PE, despite prophylaxis with low dose ASA. Studies with a larger sample size are needed to validate the role of urinary TXM as a circulating biomarker predicting suboptimal response to ASA and PE occurrence in pregnant women at high risk for PE.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


