
CO36 | Inhibitor titer at diagnosis and clinical course in acquired hemophilia A: a single-center experience
C. Simion, B. Stocco, E. Dalla Porta, E. Campello, G. Furlan, L. Spiezia, G. Saggiorato, F. Sartorello, E. Zanon, P. Simioni | Department of Medicine – DIMED, University of Padua, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background and Aims: Acquired hemophilia A (AHA) is a rare autoimmune bleeding disorder caused by neutralizing autoantibodies against factor VIII (FVIII). While the inhibitor titer is central to diagnosis and monitoring, its relationship with clinical severity and treatment outcomes remains controversial. We analyzed the experience of the Hemophilia Center at Padua University Hospital to evaluate the effectiveness of immunosuppressive and hemostatic treatments, and to assess whether baseline inhibitor titer influences clinical complications and time to remission.
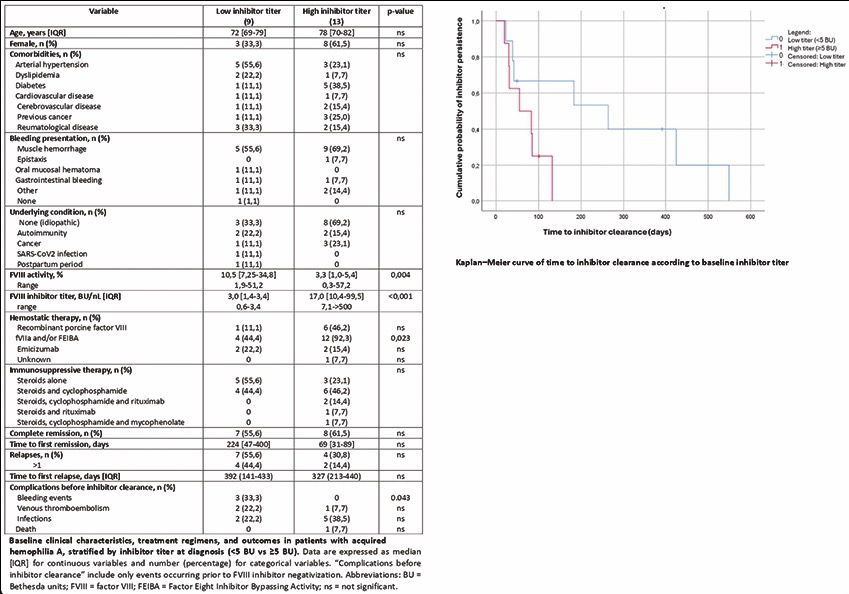
Methods: We retrospectively reviewed 22 patients diagnosed with AHA. Clinical and laboratory characteristics, bleeding events, immunosuppressive regimens, use of bypassing agents, and time to inhibitor negativization were collected. Patients were stratified by inhibitor titer at diagnosis: low (<5 BU/mL) vs. high (≥5 BU/mL). Between-group comparisons were performed using Fisher’s exact test, chi-square test, Mann–Whitney U test, and Kaplan–Meier survival analysis.
Result: The cohort included 22 patients: 13 with high-titer (≥5 BU/mL) and 9 with low-titer (<5 BU/mL) inhibitors. Baseline characteristics were comparable between groups, except for expected differences in FVIII activity and inhibitor titer (median FVIII: 1% [IQR 0.5–2.3] in the high-titer group vs. 4% [IQR 2.5–7.5] in the low-titer group; median inhibitor titer: 24 BU [IQR 10–48] vs. 2 BU [IQR 1.2–3.4], respectively). Bleeding complications occurring before inhibitor clearance were more frequent in the low-titer group (4/9) than in the high-titer group (1/13; p=0.043 by chi-square, p=0.116 by Fisher’s exact test). Bypassing agents were used more frequently in the high-titer group (12/13 vs. 4/9; p=0.023). Median time to inhibitor negativization was shorter in the high-titer group (55 vs. 264 days), with a borderline difference at Kaplan–Meier analysis (Log-rank p=0.057). No significant correlation was found between inhibitor titer and time to remission (Spearman’s ρ=–0.337, p=0.186; Mann–Whitney p=0.200). A summary table and Kaplan–Meier survival curve are provided (Figure 1).
Conclusions: According to our Center’s experience, a low-titer inhibitor at diagnosis does not necessarily indicate a milder disease course. Patients with low titers experienced more bleeding events before inhibitor clearance and showed a trend toward delayed negativization—potentially due to diagnostic delay or underestimation of bleeding risk. Conversely, patients with high-titer inhibitors might receive earlier and more intensive treatment, leading to faster resolution. While low-titer inhibitors are often perceived as less threatening, our findings suggest they may still carry a substantial bleeding risk and should not be underestimated.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


