
CO34 | Evaluation of emicizumab concentration and thrombin generation in a cohort of severe hemophilia A patients with and without inhibitor
A. Taglietti1, S. Ligia1, F. Paoletti1, R. Mormile1, E. Baldacci2, A. Chistolini1, C. Santoro1,2 | 1Hematology, Department of Translational and Precision Medicine, Sapienza University of Roma; 2Hematology, Azienda Ospedaliera Universitaria Policlinico Umberto I, Roma, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background and Aims: Emicizumab has changed the prophylaxis paradigm of hemophilia A (HA). Despite its fixed-dose, measuring emicizumab plasma concentration ([E]p) may be occasionally useful and the global hemostatic response could be monitored through Thrombin Generation Assay (TGA). Our aim is determining [E]p and TGA parameters and evaluating them across our patient (pt) cohort.
Methods: Retrospective, single-center study including 29 pts with severe HA and 6-month minimum follow-up (FU). Data were collected from clinical charts. Pts received subcutaneous 3 mg/kg emicizumab weekly for 4 weeks (loading doses, LD), followed by physician’s choice of maintenance regimen (steady state, SS). Blood sampling was performed 7 days after each LD and periodically during SS. A modified one-stage factor VIII assay was used to measure [E]p. TGA was performed by Calibrated Automated Thrombography using PPP-Reagent (phospholipids [4 uM], TF [5 pM]). TGA parameters included Lag Time (LT), Endogenous Thrombin Potential (ETP), Peak and Time to Peak (TtP).
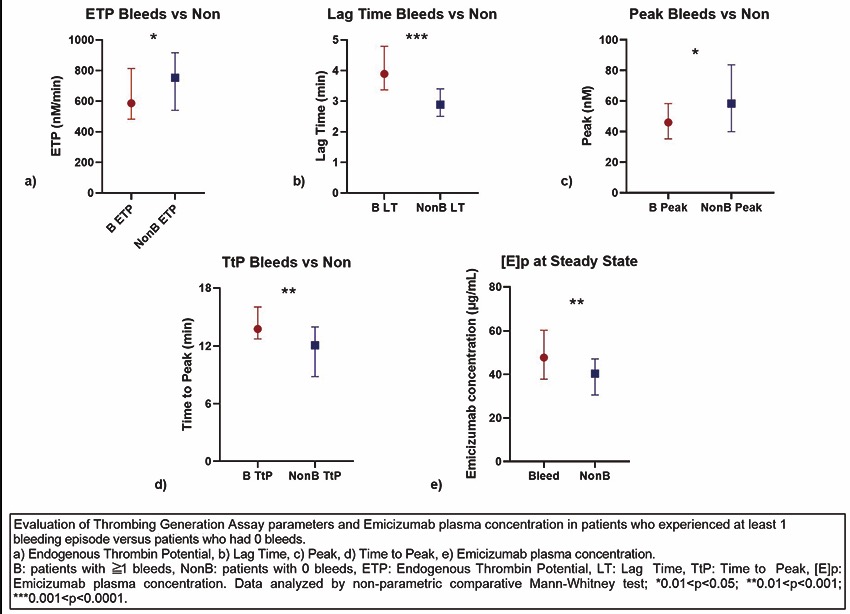
Results: 29 pts (23 non-inhibitor, 6 inhibitor). At FU, 18/29 (62.1%) pts were getting lower doses than initial maintenance dose, with a median reduction of 26.7% (range 3.3 - 33.3%) - dosage had not been adjusted to increasing weight in pts without clinical issues. [E]p was measured on 46 LD and 93 SS samples. We analyzed LD [E]p only in 16 non-inhibitor pts. As expected, median [E]p showed an increasing trend through the LD; the increase was significant between I and II LD (p=0.0095) and I and III LD (p<0.0001). At SS, median [E]p did not differ in non-inhibitor vs. inhibitor (p=0.0969) nor in pediatric (age<12) vs. adult (age>12) pts (p=0.9671). Conversely, pts who had at least 1 bleed (≧1 bleeds; 15 pts) during FU had a significantly higher median [E]p at SS than those with zero bleeds (14 pts) (p=0.0018). TGA was performed on 44 LD and 87 SS samples. TGA parameters did not significantly vary through the LD in the 16 non-inhibitor pts. Likewise, TGA parameters did not differ at SS in non-inhibitor vs. inhibitor pts. We compared TGA parameters in the pediatric vs. adult population: median ETP was significantly greater in pediatric pts (p=0,0134); other parameters did not reach statistical significance (LT p=0.30, peak p=0.07, TtP p=0.86). TGA in pts with ≧1 bleeds vs. zero bleeds showed significant differences: pts with ≧1 bleeds had longer median LT (p=0.0001), lower ETP (p=0.038), reduced Peak (p=0.0339), and longer TtP (p=0.0019). Yet, TGA parameters did not differ between pts receiving standard or underdosed emicizumab prophylaxis (p=0.59, p=0.33, p=0.85, p=0.09, respectively).
Conclusions: During emicizumab prophylaxis, [E]p increases throughout the LD until it reaches a plateau at the SS. [E]p is not affected by inhibitors or age. Lower [E]p did not correlate to greater bleeding risk, as in our cohort pts who had bleeds are unexpectedly the ones with higher [E]p. This finding may be due to a more accurate emicizumab dose adjustment - based on body weight - in the pts with a more hemorrhagic phenotype. As for TGA, parameters did not vary through the LD or in the presence of inhibitors. Yet, median ETP was significantly greater in the pediatric population. TGA parameters may also be correlated to hemostatic outcomes as a significant difference in all parameters was detected in pts with ≧1 bleeds. Conversely, we proved that a lower than standard dose of emicizumab did not affect TGA in our cohort.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


