
PO82 | Retrospective application of the TH2 score in a multicenter cohort of ITP patients: a reliable predictive tool or a score in need of refinement?
C. Giubbilei1, M. Defina2, S. Rosati3, M. Rocco3, A. Votto4, F. Simonetti5, F. Paoletti6, V. Carrai1 | 1Hematology Unit, AOU Careggi; 2Hematology unit AOU Senese; 3Hematology Unit Azienda Sanitaria Toscana Centro; 4Hematology Unit, AOU Pisana; 5Hematology Unit, Ospedale Versilia; 6Hematology Unit, Azienda Sanitaria Nord Ovest, Italy
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
Background: Immune thrombocytopenia (ITP) presents a dual risk of bleeding and thrombosis. While TPO receptor agonists (TPOra) effectively restore platelet counts and reduce bleeding, they may not fully prevent thrombosis. CV events, observed even with low platelet levels, suggest inflammation plays a secondary role. SYKi (e.g., fostamatinib, FST) may help by mitigating inflammation. The TH2 score (Balitsky AK et al., Blood 2018 ) was designed to help clinicians balance thrombotic and bleeding risks in treatment decisions. However, its use lacks international consensus, and its effectiveness in preventing CV events through tailored therapy remains uncertain. Aim: Retrospective evaluation of the TH2 score in ITP: its role in CV event prevention and therapy guidance.
Materials and Methods: We performed a multicenter retrospective analysis of 24 patients (11 females, 13 males; median age 71, range 32–90). At diagnosis: median age 63 (11–88), treatment lines 2 (1–5), platelet count 17×109/L (3–94). 19 began first-line CCS therapy. TH2 scores were recalculated with therapy changes; non-switchers were excluded. Median CV risk factors/patient: 3 (0–5).
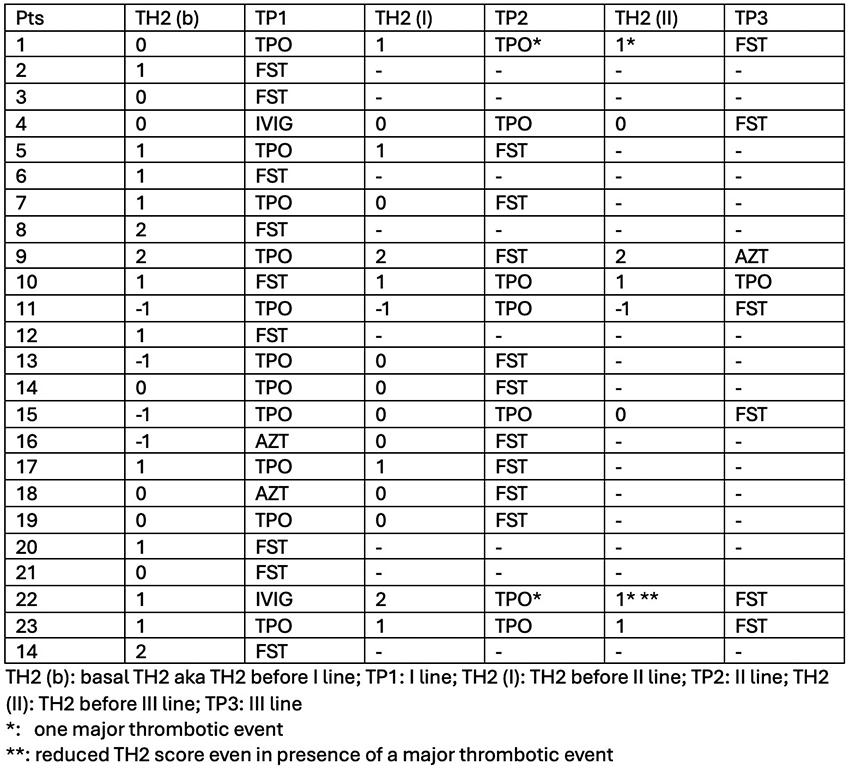
Results: At baseline, 20/24 patients had a prothrombotic TH2 score: of them 8 started TPOra, 9 received FST, 2 IVI and 1 AZT. Detailed results are in Table 1.
Conclusions: In just 3 cases (15%), an increased TH2 predicted a CV event, but the score remained unchanged; on the contrary in one instance it actually decrease after the event. However patients continued treatment safely with FST in absence of newer events. In other cases, low platelet counts likely limited score changes during therapy shifts. Although limited sample size, TH2 score didn’t optimally stratify patients, as it often indicated prothrombotic risk without translating into CV events.These findings highlight the TH2 score’s limitations in stratifying patients, suggesting the need for refinement to enhance its clinical utility in guiding personalized therapy.
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.


